Introduction:
The use of analgesia for traumatic pain in the US military has not evolved historically like other areas of trauma care. During the US Civil War and all wars up to the Afghanistan conflict in 2001, intramuscular (IM) morphine was the primary medication used to relieve severe pain. Morphine is known to be very slow-acting with a required waiting period to assess effectiveness, which can prolong the casualty’s pain. Battlefield medic/Corpsmen (hereafter Corpsmen) would then increase the likelihood of administering additional doses to manage ongoing pain at the risk of an overdose. A complication of morphine is the impediment of resuscitation efforts by its effect on decreasing blood pressure, heart rate, and respiration rate.
In the first generation of Tactical Combat Casualty Care (TCCC) Guidelines in 1996, it was recommended to discontinue IM morphine for battlefield trauma care, and to use morphine administered intravenously (IV) for rapid analgesia and improved ability to titrate the dose. Since that era, the Committee on Tactical Combat Casualty Care (CoTCCC) has had a long history with updates to the pain management section of the TCCC Guidelines. See Table 1 for a chronology of analgesia changes and updates.
Table 1. The chronology of pain management updates in the TCCC Guidelines.
| TCCC Analgesia Chronology |
TCCC Analgesia Recommendations |
1st Generation
Butler et al.
Mil Med 1996
|
Analgesia as necessary: morphine (5 mg IV)
Wait 10 minutes
Repeat as necessary
|
|
2nd Generation TCCC Update
McSwain et al
Prehospital Trauma Life Support (PHTLS) Manual 5th edition, 2003
|
Pain medications were listed in the TCCC Guidelines based on: Able to fight: Rofecoxib (50 mg po qd), acetaminophen (1,000 mg po q6 hours); and Unable to fight: morphine (5 mg IV/IO), reassess in 10 minutes, repeat dose every 10 minutes as necessary to control severe pain
|
3rd Generation TCCC Update
McSwain et al
PHTLS Manual 6th edition, 2006
Wedmore et al J Trauma 2004
Kotwal et al Ann Emerg Med 2004
Butler F. Mil Med 2007
|
The 2006 TCCC guidelines substituted meloxicam and added extended-release acetaminophen for oral analgesia for individuals who are able to fight. A new addition to battlefield analgesia was oral transmucosal fentanyl citrate (OTFC) 800 mg transbuccally for individuals unable to fight.
Mild pain and able to fight: Mobic 1 tablet (5 mg po qd), Tylenol, (650 mg bilayer caplet, 2 po every 8 hours)
Severe pain unable to fight: oral transmucosal fentanyl citrate (OTFC) 800 mg transbuccally.
IV or IO access obtained—morphine (5 mg IV/IO), repeat dose every 10 minutes as necessary to control severe pain.
|
2012 TCCC Analgesia Update:
https://www.health.mil/ Reference-Center/Reports/2012/03/08/Prehospital-Use-of-Ketamine-in-Battlefield-Analgesia
|
In 2012, The Defense Health Board recommended that DoD add ketamine to be used for analgesia to the TCCC Tactical Field Care and Tactical Evacuation Care Guidelines.
CoTCCC added IM, IN ketamine as a nonopioid option for battlefield analgesia.
|
|
2014 TCCC Analgesia Update:
Butler et al.
J Spec Oper Med. 2014
|
Triple-option analgesia was added that included one or more of three options: (1) the meloxicam and acetaminophen in the TCCC Combat Pill Pack for casualties with relatively minor pain who are still able to fight; (2) OTFC for casualties unable to fight who have moderate to severe pain, but who are not in hemorrhagic shock or respiratory distress, and are not at significant risk for developing either condition; or (3) ketamine for casualties who have moderate to severe pain but who are in hemorrhagic shock or respiratory distress or are at significant risk for developing either condition. |
2016 TCCC Analgesia Update:
Montgomery et al. J Spec Oper Med 2017
|
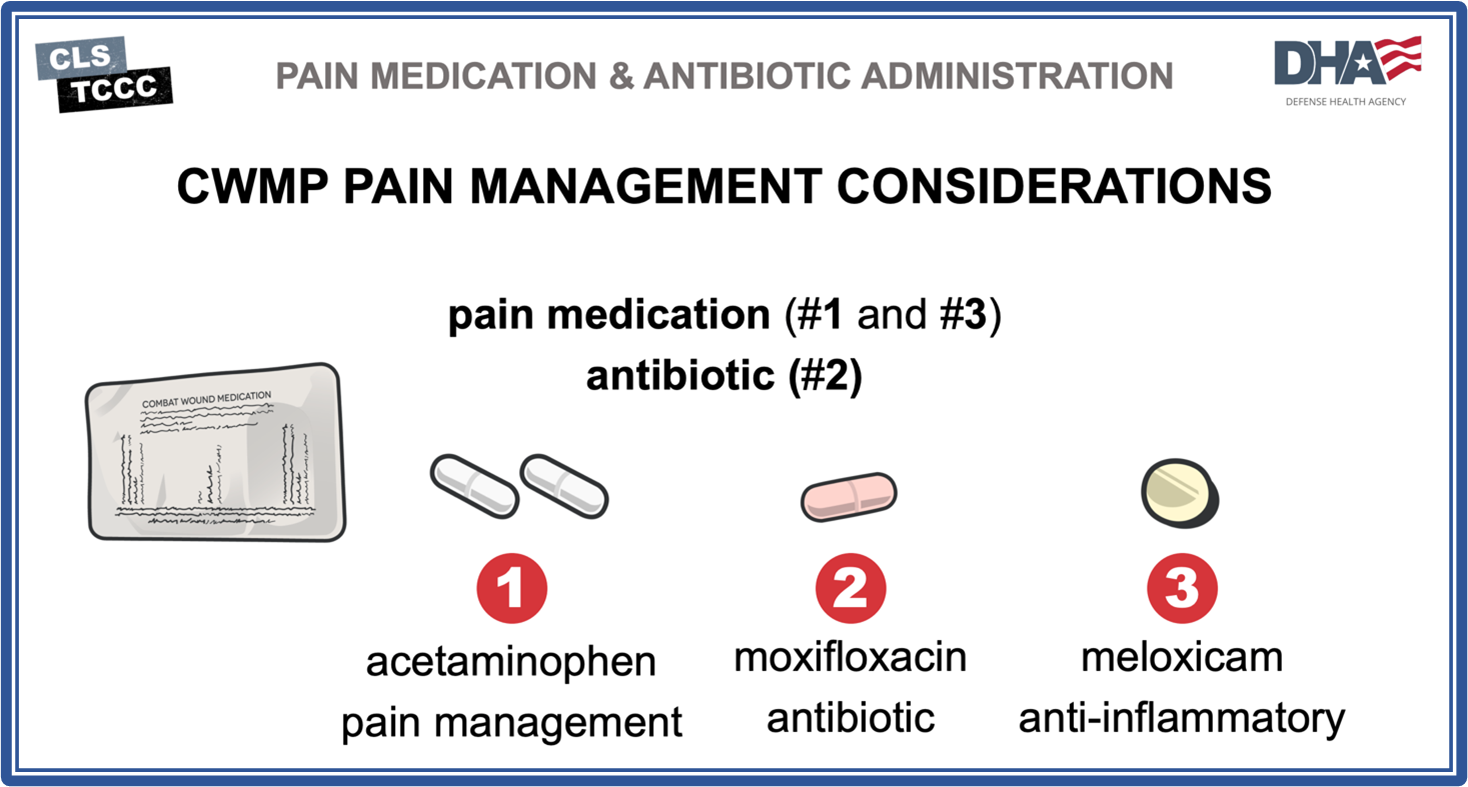
The term used previously in the TCCC Guidelines, Combat Pill Pack, has changed to Combat Wound Medication Pack (CWMP). Adopting this supply-system phrase into the TCCC Guidelines will get TCCC practitioners and logisticians to use one name for this unique combination of medicines. The recommendations for the medications contained in the package remain unchanged.
Contents of TCCC Combat Wound Medication Pack
o Acetaminophen – 500 mg tablet, 2 PO every 8 hours
o Meloxicam – 15 mg PO once a day
o Moxifloxacin – 400 mg PO once a day (antibiotic for penetrating injury)
|
2021 TCCC Analgesia Update:
Fisher et al. J Spec Oper Med 2022
|
This TCCC Guideline update addressed the following issues related to analgesia on the battlefield: 1) The development of additional pain management strategies; 2) Recommended changes to dosing strategies of medications such as ketamine; 3) Recognition of the tiers within TCCC and guidelines for higher-level providers to use a wider range of analgesia and sedation techniques; and 4) An option for sedation in casualties that require procedures. |
Background:
In 2021, the CoTCCC updated the guidelines for battlefield analgesia and sedation. There were a series of issues that justified the recent analgesia update recommendations. These were: 1) the Joint Trauma System noted some evolving trends with low rates of TCCC analgesia practice during battlefield trauma care; 2) further discussion among CoTCCC members about the prevention of post-traumatic stress and the need for additional treatment options for sedation of battlefield casualties; and 3) there are a variety of medical skill sets on the battlefield, and CoTCCC now provides trauma care recommendations for four tiers of TCCC providers. This includes administration of pain medications that range from non-medical first responders, called All Service Members (Tier 1); Combat Lifesaver (Tier 2); Combat Medics and Fleet Marine Force Navy Corpsmen (Tier 3); and Combat Paramedics, Physician Assistants and Physicians (Tier 4). See Section 10 Analgesia in the TCCC Guidelines for the current recommendations across all four Tiers of TCCC providers on the battlefield. Furthermore, the evidence that supports these changes to pain management was recently published in the Journal of Special Operations Medicine, Summer, 2022. TCCC Tier 4 providers is translated to paramedics, nurse practitioners, physician assistants, and physicians in backcountry advanced providers – see Table 2.
Table 2. New wording (red text depicts 2021 updates) for analgesia and sedation in the TCCC Guidelines for Tiers 4 providers only.
|
Option 1
- Mild to Moderate Pain
- Casualty still able to fight
|
TCCC Combat Wound Medication Pack (CWMP)
- Acetaminophen – 500mg tablet or 650mg bi-layer tablet, 2 PO every 8 hours
- Meloxicam – 15mg PO once a day
|
|
Option 2
- Moderate to Severe Pain
- Casualty is NOT in shock or respiratory distress AND Casualty is NOT at significant risk of developing either condition
|
Oral transmucosal fentanyl citrate (OTFC) 800μg
- May repeat once more after 15 minutes if pain uncontrolled by first dose
Fentanyl 50mcg IV (0.5–1mcg/kg)
Fentanyl 100mcg IN
|
|
Option 3
- Moderate to Severe pain
- Casualty is in hemorrhage shock or respiratory distress
OR
Casualty is at significant risk of developing either condition
|
Ketamine 20–30mg (or 0.2–0.3mg/kg) slow IV or IO push
- Repeat doses q 20min PRN for IV or IO
- End points: Control of pain or development of nystagmus (rhythmic back-and-forth movement of the eyes)
Ketamine 50–100mg (or 0.5–1mg/kg) IM or IN
OR
Repeat doses q20–30 min PRN for IM or IN
|
Option 4
Sedation required: significant severe injuries requiring dissociation for patient safety or mission success or when a casualty requires an invasive procedure; must be monitored and be prepared to secure the airway
if longer duration analgesia is necessary
|
Ketamine 1–2mg/kg slow IV push initial dose
- Endpoints: procedural (dissociative) sedation
Ketamine 300mg IM (or 2–3mg/kg IM) initial dose
- Endpoints: procedural (dissociative) anesthesia
If an emergence phenomenon occurs, consider giving 0.5–2mg midazolam.
If continued dissociation is necessary, move to the Prolonged Casualty Care (PCC) analgesia and sedation guidelines.
If longer duration analgesia is necessary:
Ketamine slow IV infusion 0.3mg/kg in 100 ml 0.9% sodium chloride over 5–15 minutes
- Repeat doses q45min PRN for IV or IO
- End points: Control of pain or development of nystagmus (rhythmic back-and-forth movement of the eyes)
|
Prehospital Analgesia Resources for Training:
The following are resources for TCCC pain management course materials for the four provider Tiers – see Table 3.
Table 3. TCCC training resources for pain management.
Implications for the Wilderness Practitioners:
In a recent Wilderness & Environmental Medicine Special Edition by Bennett, Butler and Wedmore, they present the translation of TCCC principles to the wilderness provider. These authors stated that the wilderness environment and the battlefield present some of the same challenges. Namely, both patient and provider are typically in remote locations; evacuation is often delayed and challenging; there are potential hazards to contend with during evacuation; resources and supplies are limited; deployment in challenging cold, hot, or aquatic environments; many first responders are not trained in trauma management. Although many of these wilderness challenges are as distinct as experienced on the battlefield, there is a huge overlap in the approach to patients in these two settings.
The translation of TCCC pain management recommendations for operational and wilderness settings first started in an article by Wedmore et al 2005. In 2014, Russel and panel members published a Wilderness Medical Society practice guideline (PG) for the treatment of acute pain in remote environments. This PG panel stated that the ideal pain medication for wilderness use should have the following qualities:1) compact and lightweight; 2) durable; 3) nonsedating; 4) wide spectrum of use; 5) biochemically and environmentally stable; 6) multiple routes of administration; and 7) minimal side effects. Furthermore, this panel recommends an escalating analgesic care plan for the typical backcountry patient. A pyramid algorithm (See Figure 1) has been created for wilderness use based on other effective algorithms. They recommend beginning care at the base of the pyramid with attention first to using the safest and most accessible interventions before any escalation to management of pain.
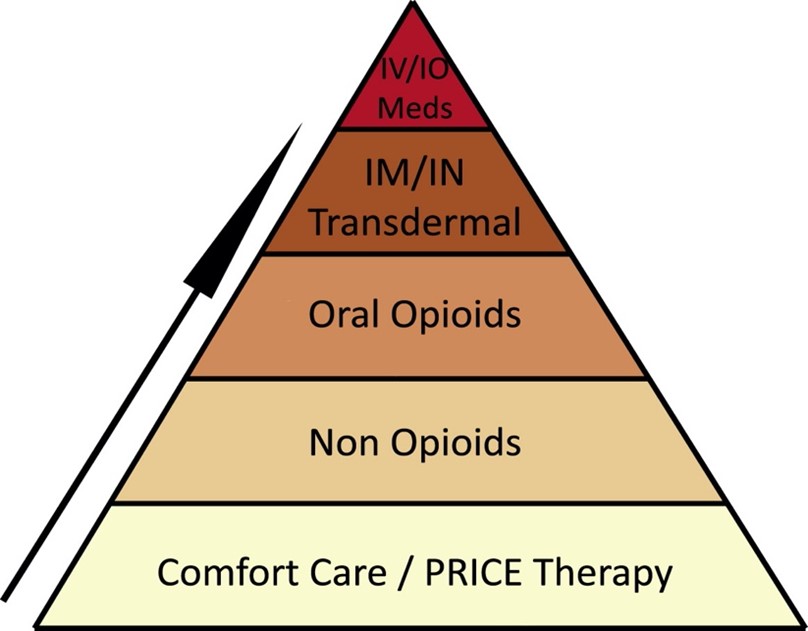
Figure 1: Escalating analgesic care for the backcountry patient.
The indications for pain control (mild to severe) in the backcountry are primarily caused by musculoskeletal injuries, including strains, sprains, dislocations, and fractures; other reasons include cold injury, i.e., frostbite, insect bites and stings, and burns. More common in mountain medicine is the management of polytrauma, e.g., falls from height, etc., that may include traumatic brain injury, spinal cord injury, thoracic, pelvic and long bone fractures with internal organ contusion or laceration. In these scenarios, IV/IO/IN opioids or ketamine are frequently used for analgesia and sedation. More recently, Wedmore and Butler in 2017 reviewed analgesia and sedation recommendations in TCCC Guidelines for translation to the wilderness environment. The Triple-Option Analgesia approach that began in the TCCC Guidelines in 2014 continues to be very applicable for the advanced wilderness provider for: 1) pain medications in the Combat Wound Medication Pack; 2) OTFC for patients who have moderate to severe pain, but who are not in hemorrhagic shock; or 3) ketamine for patients who have moderate to severe pain, but who are in hemorrhagic shock or respiratory distress, or are at significant risk for developing either condition. The 2014 TCCC Guidelines for Triple-Option Analgesia are now superseded by the pain management recommendations by Fisher et al 2022 in the most recent guideline update.
Final Thoughts:
The TCCC analgesia updates since 1996 are just one of many significant advances in the past 25+ years by the CoTCCC for managing mild to severe trauma on the battlefield. The medications in the CWMP are not novel for mild pain, but are conveniently packaged for personal injury use or for managing others with mild pain on the battlefield. The two pain medications in this pack, should be considered as essential for a wilderness medical kit. Within military medicine, there is significant experience with managing severe trauma from battlefield injury, and many years of documented effectiveness with OTFC and ketamine at the point of injury. Ketamine administration covers a wider range of indications for both analgesia and sedation. For this reason, ketamine, as a minimum, is the preferred choice for managing severe pain in a wilderness medical kit for providers with the appropriate scope of practice.