Flash Flooding Devastates the US Southwest
Lindsay Davis, DO, MPH PGY-II, Central Michigan University
Written on August 30, 2022/Volume 39, Issue 3
In the News
Some of the American Southwest’s most famous outdoor destinations including Moab, Carlsbad Caverns, and Zion National Park have faced an onslaught of flash floods over the last few weeks. Flash flooding can be particularly dangerous in the area’s many famous slot canyons. On August 22, Moab received over one inch of rain within 20 minutes, causing significant flooding within the surrounding parks and town and leading to closure of many areas. This was considered a 100-year flood (meaning 1% chance of occurring every year). This was the third flash flood in Arches National Park in the past month. Not far away in New Mexico, over 200 people were stranded in Carlsbad Caverns after a storm brought severe flooding making exits impassable. When initial evacuation efforts by the park were unsuccessful, visitors ended up having to shelter in place for several hours until the zone was deemed safe. Flash floods in Zion’s famous slot canyon known as the Narrows left many hikers scrambling for higher ground, while others were swept downstream. One missing hiker from Arizona was found dead several days later downstream along the Virgin River, suspected to have drowned in the surging waters. Multiple trails in the park remained closed for safety.
Link to Climate Change
The Southwest US is in a 22-year drought, beginning in 2000. These recent heavy rains have only made a small dent in the prolonged drought – several high-precipitation winters will be needed to help reverse the long-term trend. There has been an increase in the intensity between the wet and dry seasons, and the worsening dry seasons prevent the heavier rains of the monsoon season from being absorbed into the ground leading to more severe flooding over time. For every one degree Fahrenheit increase in temperature, the air can hold 4% more water. Moab has seen more flooding over recent months, especially after a 2021 wildfire in the surrounding La Sal mountains has affected the local terrain’s ability to retain water; rainwater will rush unhindered over the large burn scar area and into low-lying areas.
Flash Flood and Canyon Country
Canyons, ubiquitous in the US Southwest, present unique dangers to the wilderness explorer. A quick internet search will yield many fatal events due to flash floods over the past several years. One of the most notable events, known as the Keyhole Seven, occurred in 2015 when seven canyoneers died in Zion National Park during a flash flood after local storms dropped 0.63 inches of rain increasing local river peak flows from 55 cfs to 2630 cfs. Flash floods are the largest cause of disaster-related deaths in the United States. In flash floods, 90% of deaths are attributed to drowning, although trauma and hypothermia may be important factors as well. Flooding in the Southwest US is most common during the monsoon season which occurs from April to October. During these months, visitors to canyon country must pay close attention to the weather before hiking, climbing, or canyoneering. It does not need to rain in the spot where you are for a canyon to flood. In slot canyons, flash flooding, originating from much farther upstream, can overwhelm an area within minutes or even seconds. There are some hints that a canyon is about to flood: there may be smaller initial waves and water levels may rise before a large wave comes fully flooding into a canyon. Flash floods can still occur in an area where there is as little as a 30% chance of rain. Indications for a flash flood include any deterioration in weather, sudden changes of water color from clear to muddy, rising water levels, stronger currents, or an increasing roar of water. To protect yourself when in a slot canyon, seek higher ground immediately. If this is not possible, find something to hold onto such as trees or rocks. It is of the utmost importance to be prepared prior to adventuring within a slot canyon; always look ahead at the forecast, always take maps and ample food and water, have a backup plan, and always tell someone where you are going and when you expect to be back!
.png)
Carlsbad Caverns after recent rains image from NYT
Video of flooding in a slot canyon:
Lightning Kills NOLS Backpacker While Inside His Tent
Lainey Yu, DO, MS, FAWM, Wilderness Medicine Fellow, UC San Diego
Written on August 13, 2022/Volume 39, Issue 3
Twenty-two-year-old University of Colorado Boulder student Jack Murphy was killed in a lightning strike while on a backpacking expedition in Bridger-Teton National Forest on August 2. He was with a group of fourteen adults on a course with the National Outdoor Leadership Schools (NOLS), a nonprofit organization that specializes in wilderness education. Another participant on the trip was also injured but in stable condition.
According to Teton County Search and Rescue (TCSAR), CPR had been in progress for over an hour by the time their helicopter arrived, but Jack could not be revived. According to their analysis, the fatality was a random event and the group had followed best safety practices during the lightning storm, spreading their shelters apart in an area of low-lying terrain amongst trees of even heights. The victim was inside his tent at the time of the strike.
According to KC Bess of TCSAR, the two students struck by lightning were 25 yards apart and may have been affected by a shock that traveled through the ground, also known as a ground current. The other student was reported to have burns and “nerve issues” that can be common after a lightning strike.
Lightning can strike people in multiple ways:
- Direct Strike: lightning extends from the sky directly down to a person, usually in an open area
-
Side Flash/Side Splash: lightning first strikes a taller object nearby, then jumps to the victim, often when a person is near a tall tree or other object
-
Ground Current: lightning strikes an object and travels along the ground via conductive materials (ie, rainwater) and spreads to a larger area, affecting everything touching the ground (commonly seen in mass livestock deaths)
-
Conduction: lightning strikes a conductive object or surface (ie, metal, water) that a person is in contact with at the time of the strike, thereby absorbing the current of the strike
-
Streamers: lightning strikes a nearby object and the charge spreads to a person in a nearby area with positively charged ions which carry the charge of the strike

Types of Lightning Strikes. Source: https://www.weather.gov/safety/lightning-struck
Lightning Position/Crouch:
Of note, the lightning position has not been proven to lower the risk of a lightning strike and the National Weather Service stopped recommending it in 2008. However, it is still valuable to review the theory behind the position in situations where definitive shelter is not an option. The lightning position is where your feet are close together (to minimize the distance a ground current would travel) on nonconductive material (to decrease the likelihood that a ground current will enter you) and you are crouched low to avoid the chance of side splash or streamers.
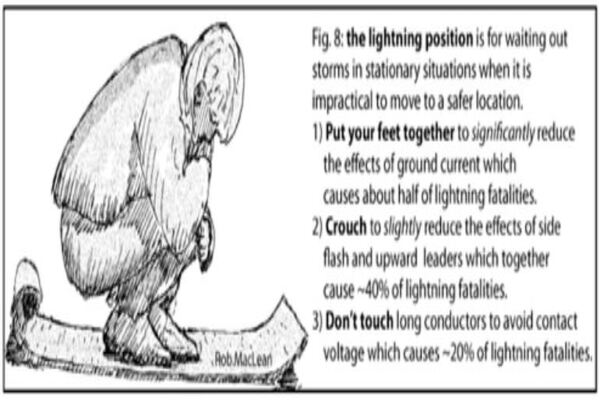
Lightning Position. Source: NOLS.edu
Reverse Triage:
If your group is unlucky enough to be struck by lightning and there are multiple victims, the role of reverse triage applies; the victims that appear to be dead (and would typically be given a black tag) should be attended to first because the chance of getting return of spontaneous circulation (ROSC) is high within the first few minutes of a lightning-induced cardiac arrest. If available, an AED can be used to detect shockable arrhythmias.
Common Lightning Injuries:
- Keraunoparalysis: transient paralysis secondary to vascular spasm from autonomic overstimulation. Presents as a cold and mottled limb with neurologic and pulse deficit. Often resolves within a few hours. Spinal precautions should be maintained until definitive diagnosis can be made.
-
Lichtenberg Figure: transient red marks on the skin from suspected damage to superficial blood vessels from lightning being conducted on the surface of moist skin, usually appear one hour after a strike and disappear within 24-48 hours.
-
Tympanic Membrane Rupture: rupture of the eardrum from damage to small vessels of the tympanic membrane as they conduct electricity.
-
Exploding Clothes: lightning can superheat the moisture on the skin causing it to rapidly vaporize and cause a steam explosion that can blow off clothing.
-
Burns: any conductive items (watches, jewelry, belts) can cause contact burns and should be managed as thermal burns.
Prevention:
It is always a good idea to educate yourself about lightning when going outdoors in areas that are prone to thunderstorms and have a plan for taking shelter if you are caught in a storm. According to the WMS Practice Guidelines for the Prevention and Treatment of Lightning Injuries, buildings or vehicles provide the greatest shelter from lightning. If unable to seek definitive shelter, remove any metal objects (Grade 1C), assume the lightning position (2C) and spread your group out by >20ft (1C). Avoid peaks and ridgelines (1C) and exit the water (1C).
Recent Floods in Eastern Kentucky: A Local Student’s Perspective on How to Prepare
Rachel Chauvin, OMS-III
Written on July 29, 2022/Volume 39, Issue 3
On July 27, a torrential downpour and the resulting 1000-year flood, left eastern Kentucky mourning the loss of at least 16 residents and many more unaccounted for. The record-breaking rain left many people waiting for help on their rooftops. Local search and rescue teams as well as many local Good Samaritans jumped into action to assist their neighbors and families. President Biden declared a major disaster for Kentucky on Friday, July 30 in addition to the twelve counties and two major cities also declaring their own individual states of emergency.
As a third-year medical student in Pikeville, Kentucky―which neighbors the areas affected by the floods―I was unable to reach the clinic where I was assigned to perform my rotations. Roads were unpassable due to the water and debris from the landslides; classmates from neighboring towns reported that their apartments and automobiles were completely flooded leaving them stranded waiting for help. The volunteer search and rescue team I am a member of, Wolfe County SAR, assisted 80 people out of the flood areas during a 17-hour operation. My medical school’s organizations, local businesses, churches, and city officials are currently coming together to assemble supplies and volunteers to aid those affected by the floods.
.jpg)
View of road leading to the clinic.
.jpg)
Local town effected by floods.
Local town effected by floods.
Here are a few important guidelines to help prepare for the upcoming flood season:
- Know the location of your local town emergency shelters and know local authority’s phone numbers.
-
Assign a family member or friend as an out-of-state emergency contact in case your family is separated.
-
- Be prepared to shut off electricity, gas, and water
- Install sump pumps with a back-up power supply
- Install backflow valves to drains, toilets, etc., to stop floodwaters from flowing into the home
- Prepare an emergency kit
- Flares: important for signaling for help, especially if your home is isolated from others (a common occurrence in Appalachia)
- Flashlights with extra batteries
- Contour and terrain maps that show areas that are higher in elevation
- Tools including a saw or axe to clear debris that may block exit routes during a heavy rainstorm
- Cold packs: flood season is usually Spring and Summer when temperatures can reach 80° to 90° degrees F with high humidity in some regions
- Waterproof clothing, rubber boots, and heavy-duty gloves to protect yourself from flood water which can contain contaminants, sharp objects, electric wires, and other hazards - Insect repellant, pants, and long-sleeved shirts to combat potential mosquitos accumulating in stagnant water
- Prepare an emergency water supply: one gallon per person (and pet) per day for three days and non-perishable food.
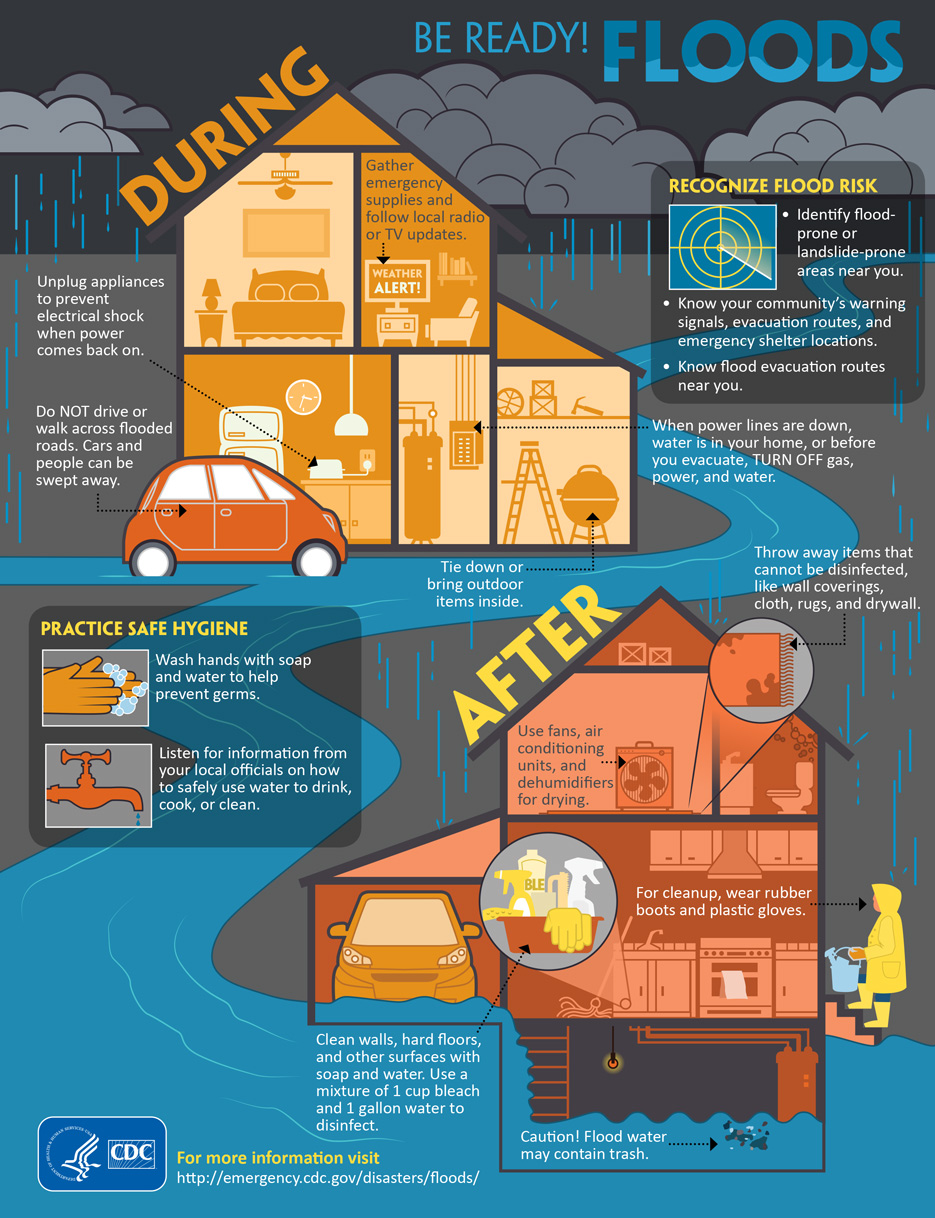
Flood Preparedness Source: CDC
How to prepare during an active flood warning:
- Have an evacuation plan, including routes and alternatives
-
Fill up the fuel in your vehicle ahead of time
-
Have important documents prepared and ready to go in case of evacuation (IDs, Passport, insurance, etc.)
-
Check the news and radio for updates and pay attention to phone alerts
-
Prepare to turn off the electricity, water, and gas in your home
-
If internet is available, check for road closures
-
Have a separate power source to charge phones and other communication devices
-
If caught in a flash flood, proceed to higher ground when safe to do so
-
Avoid touching or entering flood water, as it is unpredictable and may contain active live wires from downed powerlines, mobile objects large enough to cause crush injuries, etc.
-
Do not attempt to cross or drive through flooded roads
-
Practice safe hygiene. Wash hands with soap and fresh wate
After a flash flood:
- Throw anything away that cannot be disinfected including drywall, rugs, couches, etc.
- Clean walls and hard surfaces with cleaner containing bleach
-
Wear rubber gloves and boots while cleaning
-
Make sure any food or water in the home has not been contaminated by flood water before consuming
Ways to donate to this cause:
New Drug Aims to Change How We Treat Venomous Snake Bites
Sheri Li, MD, PGY-I
Wellspan York Hospital, Emergency Medicine Department
Written on July 21, 2022 | Volume 39, Issue 3
As summer hits full swing and more people venture outside for outdoor activities, ED visits for snake bites often increase as well. Venomous snake bites affect an estimated 2.7 million people around the world each year and may lead to death or disability in nearly half of a million people. The current treatment for many venomous snake bites includes intravenous antivenom therapy directed to the specific family of snake, which in the United States is usually pit vipers and coral snakes. The goal of antivenom therapy is administration within 30 minutes of the bite, as the venom can spread very quickly once inside the body. Unfortunately, timely administration is often not possible; 75% of the deaths from snake envenomation occur in the prehospital setting as antivenom may not be readily available.
Additionally, antibody therapy can be very expensive and patients often require multiple doses to sufficiently neutralize the venom. A single antibody course for one patient may cost over $100,000, without including the cost of hospitalization. Total hospital bills have been reported to be as high as $244,995. For a patient without insurance, this type of treatment is not affordable.
Outside of the US, snake bites are prevalent, under reported, and often fatal, such that the WHO has designated snake bites as a neglected tropical disease. Thus, it was big news in March 2022, when the FDA approved a new Fast Track designation for a novel drug to hopefully change the paradigm for venomous snake bite treatment. This new drug, called varespladib, has two novel attributes: (1) it is administered as a pill, and (2) it aims to be universally effective for all venomous snake bites. Its mechanism of action is to target secreted phospholipase (PLA), a protein which is present in more than 95% of snake venoms.
The BRAVO (Broad-spectrum Rapid Antidote: Varespladib Oral for snakebite) study is a randomized, double-blind, placebo-controlled trial that includes 12 centers worldwide, six of which are in the United States. Study participants all receive the standard species-specific antivenom treatment and then randomized to receive either varespladib or control. The primary study endpoint is to assess for pulmonary, cardiovascular, hematologic, and nervous system symptoms using the snakebite severity score (SSS). Currently, seven patients have been enrolled and treated. Once completed, researchers expect their data to include bites from pit vipers, coral snakes, monocled cobras, Russell's vipers, and other less common venomous snakes from across the world.
If proven to be effective, this drug could increase access to snake bite treatment in rural areas by having a universal treatment for all snake bites, eliminating the need for species-specific antivenom. It may also eliminate the need for special storage requirements that could be difficult to maintain in rural areas. Additionally, it may even decrease the amount of analgesia required and reduce the hospital length of stay.
While this drug is promising, there are some drawbacks to the study. First, the study is only aiming to enroll 110 patients from centers in the United States and India, limiting the power of the study and inclusion of different toxins. Second, the participants in each group are not matched with controls receiving bites from the same species of snake, making the analysis less robust. However, this study has the potential to be a major step in treating snake bites in rural, underserved populations with high mortalities such as in Nepal or various countries in sub-Saharan Africa. If approved, this drug could present a solution to some of the biggest barriers to snake bite treatment.
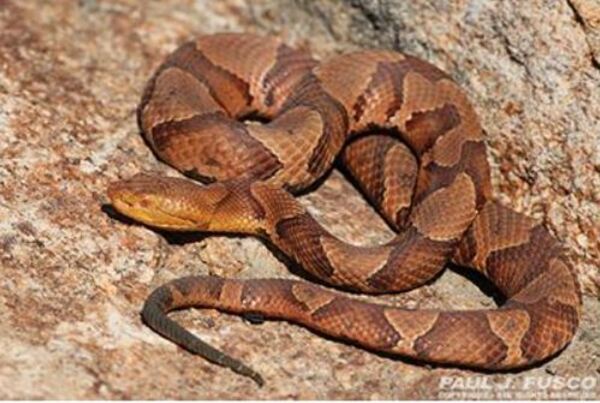
Copperhead snake, a species in the pit viper family.
Three Yellowstone Visitors Gored by Bison in Four Weeks
Mary Rosegrant, DO, PGY-V
UT Health Science Center San Antonio
Written on July 6, 2022 | Volume 39, Issue 3
With pandemic visitation restrictions eased and tourist numbers on the rise, the 2022 season has already seen three bison attacks at Yellowstone National Park.
The first event occurred on May 30 near a boardwalk at Black Sand Basin.
According to reports, a 25-year-old female from Ohio approached a nearby bison coming within 10 feet before the animal gored the woman, tossing her 10 feet into the air.
She sustained a puncture wound and other injuries and was transported to a hospital for further evaluation and treatment.
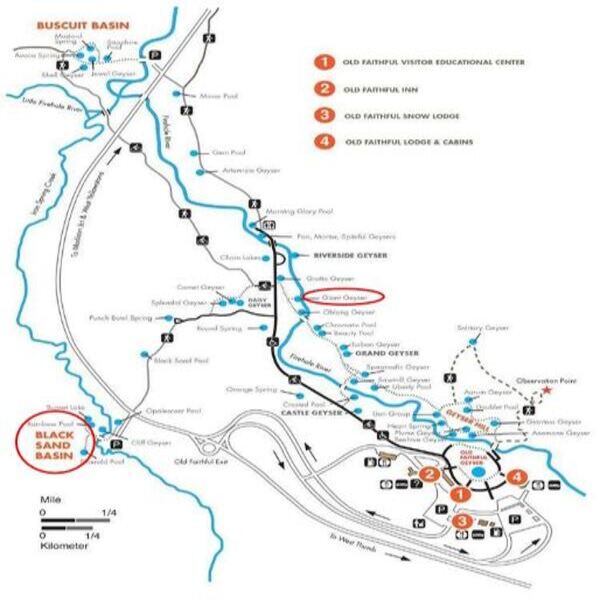
Figure 1: Map of several of this year's bison goring locations.
On June 27, a 34-year-old Colorado man and his family were walking along a boardwalk near Giant Geyser when a bison charged their group. The group did not attempt retreat and the man was gored, resulting in an upper extremity injury requiring transport to an Idaho hospital. Just two days later, a third visitor, a 71-year-old female Pennsylvanian and her daughter were returning to the Storm Point trailhead near Yellowstone Lake when they unknowingly approached a male (bull) bison. It charged the woman, leading to non-life-threatening injuries and ambulance transport.Yellowstone National Park is home to the largest herd of bison (Bison, bison; also known as buffalo) in North America, numbering around 5,450 as of summer 2021. On the brink of extinction at the turn of the 20th century, conservation efforts have since seen the population of North America largest land mammal steadily rise, with over 30,000 bison now living in wild herds in multiple states and over 400,000 raised as livestock each year according to NPS data.

Figure 2: Some of Yellowstone's many bison approaching a boardwalk.
Boasting the only herd known to have been in existence since prehistoric times, Yellowstone has long been a favorite destination for sightings of these majestic creatures. Consequently, the park sees many injuries at the hooves of bison, usually as a result of visitors trekking too close.
According to park officials, bison are the cause of the majority of animal-related injuries at Yellowstone. Though these attacks are rarely fatal, they can cause serious injuries and lead to costly medical care. Though there is, on average, at least one goring per year, there are periods over which the park has seen increased interactions between bison and tourists. During a particular three-year span in the 1980s, 33 bison-related injuries were reported, which led to extensive efforts at educating park visitors on the dangers of approaching bison, along with the implementation of warning signs throughout the park. As bison are free to roam the extensive public lands, they are often seen near major roads, trails, and geyser basins, where the majority of gorings have occurred. Visitors are warned to maintain a distance of at least 23m, or the distance of a tennis court, away from bison to decrease perceived threat and chances of attack.
.jpg)
Figures 3 and 4: NPS infographics educating visitors on appropriate distances from wildlife.
There was also an increase in attacks from May-July of 2015, during which five bison-related injuries were reported. This increase led to analysis as to what characteristics may have contributed. Though some instances occur merely as a result of chance interactions or inattention, many are related to attempts at taking close-up photos of the beasts, including so-called selfies. Most encounters have occurred with people far closer than the recommended 75 feet, with the 2015 photography-related attacks reporting distances of only 3-6 feet.
Figure 5: Example of poor selfie-stick etiquette.
Bull bison grow up to 6-8 feet tall and weigh up to 2,000 pounds; females (cows) up to 1,000 pounds. Their mating period runs parallel to peak visitor season at Yellowstone (late July-August), and cows give birth late April-May. Bison can reach a maximum running speed of 30-35 mph, about three times faster than most humans. If a bison is grunting, hoofing the ground, or showing other signs of agitation, it is advised that those nearby turn and retreat away. Do not attempt to stare down the bison or stand your ground as this could be perceived as a threat and incite the bison to charge. Bear spray can also be used if it is at hand. As a general rule, the NPS advises that visitors always stay 25m from all large animals, including elk, bighorn sheep, deer, moose, and coyotes, and at least 100m from bears and wolves.
Bear Attacks: Prevention and Protection
Erin Hillis, PA-C
Written on July 3, 2022 | Volume 39, Issue 3
9/7/21 Update: An initial version of this article has been updated with clarified information regarding responses to bear attacks.
Bear attacks have become increasingly common throughout the country this summer. On June 24, a mother and her daughter were camping near Trinidad, CO, when a bear stepped on and popped a beach ball and woke the two-year-old girl who began crying. The mother went to check on her daughter and brushed the side of the tent when the bear swatted and scratched her head. The mother sustained superficial scratches and the bear was never caught. In another incident near Anchorage, AK, in early May, several soldiers from Joint Base Elmendorf-Richardson were scouting a training area west of the regional landfill when the group came upon a brown bear den with a mother and two cubs. The group was attacked without warning: one paratrooper was killed and another injured. Another attack on June 16, near Lake Tahoe, occurred as a woman was putting her garbage out and as she re-entered her home, the bear was already inside and scratched her face and knocked her to the ground. Most bear attacks occur when they are searching for food or are protecting their food, cubs, or territory. Preparation is key in these situations.
While human-bear encounters have increased in frequency over the years, there are several steps one can take to stay protected when in the wilderness. If you are entering the backcountry, it is important to know where it is common to find bears in their habitat. Proper storage of food and trash, including all packaging, toiletries, and scented items, is a key step in keeping a bear from wandering into your campsite. The best way to store these items is in a bear-resistant food container or a food locker. The container must be closed and locked, even while you are at the campsite. The container should be placed away from water sources and on the ground in a flat, level area 30m or more from the campsite. Do not hang anything from the container, but clean pots and pans may be placed on top that can act as an alarm signal that a bear is near the container. Many camping areas, including US National Parks, have food lockers available to campers, as hanging food is no longer a reliable option. While this is the least effective option, if needed, all scented items can he hung in a bear bag approximately 4m off the ground and 50-100m from sleeping areas.
While entering the wilderness, one should be aware of their surroundings and avoid any areas that have signs of recent bear activity, such as footprints, rub trees, scat, large areas that are dug up, freshly broken logs, or any signs of a carcass. To ensure you do not surprise a bear while traveling, always be alert of your surroundings and talk at different intervals to provide noise. Talking identifies us as humans and bears will naturally avoid this sound. While these are preventative strategies, a bear encounter could still occur. Bears may act defensively if startled. Put your arms in the air and speak in a low tone to identify yourself as a human. If the bear approaches, do not run, as the bear may chase you. If you are actually attacked by a bear, recommended responses may differ based on species. If you are assaulted by a black bear or polar bear, it is best to fight off the bear- when these bears attack, it is often predatory. If attacked by a brown bear (including grizzlies), experts recommend falling prone to the ground, spreading your legs to prevent being turned over, and covering your neck with your hands until the bear has retreated - these are often defensive attacks. Predatory attacks are rarer but can be more worrisome. Bear spray can be effective in this situation: aim for the eyes, nose, and face of the bear and throw rocks and sticks if needed. The active ingredient in bear spray is oleoresin capsicum (OC) and has been found to be very effective at deterring bear encounters and is the recommended deterrent by bear experts. These sprays are easy to use but reviewing proper use before a wilderness trip can be beneficial for effective outcomes. While bear attacks occur all over the country, the best way to keep yourself safe is by making sure you have prepared and researched your camping or hiking area and decreasing strong odors by properly storing your food and trash.
.png)
How to identify a grizzly (brown) versus a black bear. Source: Bearsmart.com

How to use bear spray when a bear is approaching. Source: udap.com

Bear walking with cub in Yellowstone National Park. Source:NPS/Jim Peaco
Gastrointestinal Illness in the Grand Canyon
David Gordon, W-EMT, EDAC, MS-I
MS2, Sidney Kimmel Medical College, Thomas Jefferson University
Written on June 27, 2022 | Volume 39, Issue 3

Typical kitchen on a river trip, Hatch River Expeditions
How can gastrointestinal infections be controlled in the backcountry? Gastrointestinal illness, often associated with diarrhea, is one of the most common medical issues encountered in the backcountry and the second most common complaint by hikers on the Application Trail. Limited opportunities for handwashing, close proximity between trip members, and challenges in water purification may contribute to promoting transmission.
In April and May 2022, Grand Canyon National Park announced reports of gastrointestinal illness among >150 private and commercial river rafters and back-country campers. Eight trips had confirmed cases of norovirus infections. As the most common cause of gastroenteritis in the United States, norovirus can spread quickly via consuming contaminated food or water. In the Grand Canyon, similar outbreaks were observed in 2005, 2010, and 2012.
Even a low viral load of the norovirus has high transmissibility rates. Norovirus symptoms include acute onset vomiting, watery diarrhea, nausea, and stomach pain. Infection can lead to severe dehydration- a potentially life-threatening hazard in the backcountry. The extreme temperatures (often >110 ºF in the inner canyon), dry heat, lack of shade, and limited potable water sources amplify these effects.
The CDC general recommendations to prevent transmission of norovirus and other fecal-oral pathogens include:
- Proper hand hygiene
- Safe food preparation and handling practices
- Avoid preparing food for others when sick
Within the backcountry, handwashing becomes a critical measure. Hand sanitizer is easy to include with supplies and many types have been shown to be effective against norovirus transmission. However, the CDC still recommends handwashing with soap and water as the best method against diarrhea-inducing pathogens, including norovirus. In large backcountry group settings, trip organizers should make provisions for a backcountry handwashing station.

Example of river trip handwashing station
These stations typically include a foot pump to move fresh water through a faucet and a supply of soap. The station(s) should be located near the makeshift kitchen and toileting facilities (aka groovers). Often consisting of a bucket, PVC tubing, bulb, and hose clamp, these stations can be a suitable and simple setup for each site (assembly guide, YouTube video guide). Biodegradable phosphate-free soaps are available to reduce environmental impact.
Proper handwashing is critical across each stage of food handling and preparation, which can become challenging when food is brought into the backcountry. Following the 2005 Grand Canyon norovirus outbreak where over 100 rafters were infected, a case-control study with a traceback investigation identified a food handler, who recently had gastroenteritis, that had sliced deli meat for the trip with bare hands in a meat processing facility. While a causative agent for the 2022 outbreak has not yet been identified, handwashing remains a proven control method to combat norovirus, especially in the backcountry setting.
Another Tragic Colorado River Drowning
Brad L. Bennett, PhD, Paramedic, MFAWM / Military & Emerg Med Dept, USUHS
Thomas Myers, MD / Medical Advisor for Grand Canyon National Park
Written on June 20, 2022 | Volume 39, Issue 3

A view looking upriver from Pipe Creek Beach. NPS File Photo/M. Quinn
The National Park Service (NPS) released a statement that on June 11, at approximately 2:00 p.m., a 47-year-old female, Sheetal Patel from Chattanooga, Tennessee, was caught by the Colorado River currents and drowned in Grand Canyon National Park. Proceeding this tragedy, she had hiked (7.6 miles) down the Bright Angel Trail to the Colorado River at the mouth of Pipe Creek (River Mile 89.6). She was meeting a commercial river boat at Pipe Creek Beach to begin a multi-day trip.
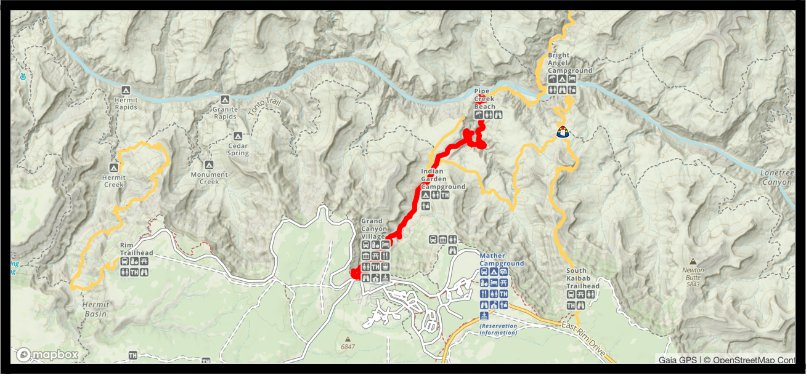
Bright Angel Trail (in red) from the Grand Canyon Village to the Colorado River.
After several hours hiking in temperatures
exceeding 100°F, she began cooling off on the river edge and was caught in
swift current and swept into the Pipe Creek Rapid (Class III). She was not
wearing a personal flotation device (PFD). River guides launched their 33-foot
pontoon motor rig to chase after her and upon reaching her found her
unconscious. CPR was initiated after pulling her from 50°F water. At the same
time, guides contacted Grand Canyon Regional Communications via satellite
reporting the mishap and that CPR was in progress. The NPS EMS dispatched
search and rescue personnel by helicopter and were on scene in less than one
hour to assist by providing advanced life support measures. Unfortunately,
resuscitation efforts were unsuccessful and the NPS medics pronounced her
deceased.

Some visitor warnings at Pipe Creek Beach.
Two other river drowning have occurred recently. Mary Kelley, a 68-year-old, died from drowning on the ninth day of a boating trip through the canyon after falling into Hance Rapid (Class V) and drowned despite wearing a PFD. Margaret Osswald, a 34-year-old, fell 20 feet to her death while on the river. For many, a rafting trip down the Colorado River is on their bucket list, but rare events like these can quickly turn into tragedy.
Initiating medical management of a drowning victim in an austere environment is extremely challenging. The WMS practice guidelines for the treatment of drowning victims recommend:
- Safety of rescuers is paramount
- Aggressively treat hypothermia
- Rapid reversal of hypoxia with effective airway management and CPR
- Use of high-flow oxygen with positive-pressure ventilation if available
- Call for evacuation and medical support
A recent WMS Magazine article discussed the risk of death on the Colorado River. There were 22 deaths out of 330,000 river runners (2010-2020). This figure includes all causes of death on a river trip, e.g., drownings, falls, etc. This equates to one death (all-cause) out of 15,000 river trip runners. Of the thirteen drownings that were reported, seven deaths occurred after a boat flipped in the rapids and the other six drownings occurred on the riverbank when victims fell or stepped into the river current without wearing a PFD. Two drownings were alcohol-related. When excluding deaths from modifiable behavior (e.g., not wearing a PDF) the risk of an on-river drownings is approximately one death out of 50,000 for all Colorado River runners. Numerous river drownings involve canyon hikers too. Every year, hikers become victims to river currents, cold water, and unexpected changes in terrain and depth. Whether hiking down to the river, rafting, or kayaking, it is essential to understand river safety. It is highly recommended to avoid wading into the river if there is swift current. In calmer sections, such as eddies, avoid going beyond knee deep or swimming without a well-fitted PFD. Near the edge of the eddies the river current can be overwhelming due to the average elevation drop of 10 feet per mile. If you do end up in the swift water current, get into the defensive swim position (i.e. body surfing on your back) and learn how to look for and swim into eddies to exit the river.
Safety Guidance On or Near the Colorado River:
- Use a buddy system near river edge and while wading.
- Avoid wading beyond knee deep, even in eddies, without a well-fitting PFD.
- Excessive alcohol and rivers don't mix well - avoid overindulgence.
- Do not attempt to cross or swim in the river.
-Be wary of weather changes that can result in flash flooding from side streams flowing in the river.
- While on-river, all boaters should remain within eyesight and keep relatively close in case of emergencies.
- Avoid jumping from cliffs into the river or side steam pools unless water depth is known and always wear a properly-fitted PFD.
- If you end up in swift water with a PFD, get into a defensive swim position.
In summary, many Colorado River drownings at the river edge are from modifiable behaviors. The NPS also provides many online resources on water hazards and river and stream safety for the Grand Canyon and other NPS water sources.
Medicine in a Changing Climate
Brennan Enright, MS-IV
University of Arizona College of Medicine
Written on June 18, 2022 | Volume 39, Issue 2
As temperatures climb across the planet, wildfire seasons get longer, storms get stronger, and sea levels rise, climate change continues to pose problems throughout our lives. Industrialization has completely changed the environment and projections for the future are rarely optimistic. The global temperature has risen 1.1°C since pre-industrial times. Most experts agree that limiting total warming to 1.5°C would avoid the most severe effects, however, without significant changes in policy and habits, the current trajectory puts global warming at 2.5-2.9°C by the end of this century.
The dire impacts of climate change on health led the WHO to declare in 2015 that climate change is the greatest threat to global health in the 21st century. The changing environment has, and will continue to have, huge impacts on human health a relationship explored in the study of climate medicine.
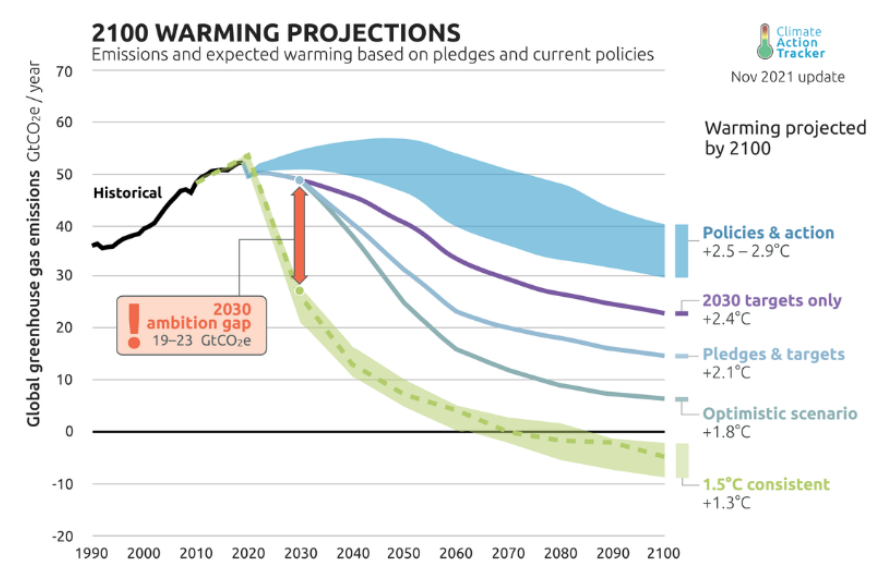
Projections for future greenhouse gas emissions and warming based on current policies, NDC 2030 targets, and net zero targets. Projections by climateactiontracker.org
A recent review article in the New England Journal of Medicine discusses specifically the ramifications of climate change on children's health. The review discusses how increasing heat waves have been associated with increases in the likelihood of preterm birth, low birth weight, pediatric kidney disease, and heat-related deaths in student athletes. Additionally, climate-intensified weather events such as flooding and hurricanes displaced over 900,000 children in the U.S. in 2020 alone, disproportionately affecting low-income communities. Wildfire smoke, like heat wave exposure, is associated with preterm birth and low birth weight as well as asthma exacerbations, bronchitis, and pneumonia in children. Additionally, vector-borne diseases, such as malaria, dengue, Zika, and Lyme, have expanded their range with outbreaks of Zika previously limited to equatorial regions appearing in Florida and Texas in 2016, and Lyme rates have increased countrywide.
Similar trends are seen among adults. A synthesis of systematic reviews from 2021 looked at the links between numerous health problems and climate change. The transmission of infectious diseases, both vector-borne and food- and water-borne, has been affected by rising temperature and humidity in numerous studies. Increasing precipitation was linked to an increase in vector-borne disease and a decrease in water-borne diseases. Temperature and humidity were also linked to increases in heat stroke, respiratory diseases, allergies, and even myocardial infarctions. Decreased air quality due to air pollution or wildfire smoke was proportional to increasing incidence of asthma, COPD, and overall lung disease. Mental health outcomes, such as hospital admissions and suicides were also linked to increased temperatures. Taking a broader view, the study even found that all-cause mortality was consistently associated with higher temperatures.
As these issues continue to impact our patients throughout the world, field-specific training opportunities have been established. In 2017, the first Climate and Health Fellowship for physicians was started at the University of Colorado and another has now opened at Beth Israel Deaconess Medical Center. These fellowships provide physicians from many specialties with training to be advocates in climate policy. Regardless of field or specialty, health care providers may be seeing more patients affected by climate change. In climate health, patient care consists of not only treating patients with heat stroke, pulmonary exacerbations, or those displaced by natural disaster, but also by being climate advocates on a national and international level. Health care professionals are seeing these problems first-hand and have an invaluable perspective to share with the world to help bring about necessary change.
Eva the Maligator Hero Dog Saves Owner in Mountain Lion Attack
Sarah Spelsberg PA-C, FAWM, FEWM, MS-III
Written on June 17, 2022 | Volume 39, Issue 2

Eva, the Maligator, as she was known, enjoying being outdoors before the attack. Instagram @eva_the_mal
A two-year-old Belgian Malinois named Eva, hailed a hero for saving her owner from a recent mountain lion attack in Northern California, died Wednesday, June 8, of injuries sustained during the attack. Eva suffered skull fractures and punctured sinuses among other injuries. The saga has been outlined on social media and has become international news.
Eva was hiking with Wilson near the Trinity River in Northern California on May 16 when a mountain lion charged Wilson ripping her jacket and scratching her shoulder. Eva subsequently attacked the mountain lion, the wild cat eventually gaining a grip on Eva's head. Despite throwing rocks and sticks at the mountain lion, Erin was not able to get the lion to release her dog. Wilson ran to her truck to get help and flagged down passerby Sharon Houston. With a tire iron, PVC pipe, and pepper spray the two women were able to eventually scare off the lion. Once freed from the lion's grasp, Eva was able to run back to Wilson's truck. Wilson told The Sacramento Bee, at first, I was like, wow she's ok. But when I looked at her closer, I realized that she had a couple of puncture wounds on her face. And she just had a lot of blood coming out of her mouth. Wilson drove Eva ninety miles to the closest emergency veterinarian.
Initially, Eva began to steadily improve and a fundraising account was set up to help cover the veterinary costs. On the weekend of June 4, Eva started seizing and on Wednesday, June 8, she passed away. Eva is being hailed a hero for her bravery in saving the life of her owner during a harrowing mountain lion attack.

gofundme.com/f/hero-dog-saves-me-from-mountain-lion-attack
The Belgian Malinois breed was initially used to herd sheep. Their intelligence, loyalty, and bravery has expanded their work into the military, police, and anti-poaching teams. A Navy SEAL Belgian Malinois is credited with assisting in the takedown of Osama Bin Ladin. Another Belgian Malinois received awards for the apprehension of 115 poachers as part of an anti-poaching team in Kruger National Park. The Malinois has been called a game changer in the anti-poaching efforts in Africa. The breed has been featured in films such as Max (2015) and Dog (2022).
Mountain lions are also referred to as cougars, pumas, mountain cats, catamounts, and panthers. As of 2019, a total of 126 mountain lion attacks on humans have been reported in North America, 27 of which were fatal (including the 2018 attack of two Seattle cyclists). Mountain lions frequently attack the head and neck, as happened with Eva, and the puncture wounds and strength of their jaws can inflict serious injuries. Mountain lions will kill their prey through head trauma, tracheal injury, cervical spine injury, or massive hemorrhage. Attacks are fortunately rare occurrences and humans are more likely to be killed by a bear, lightning, or even a bee. While the presence of dogs is a possible trigger in bear attacks, trained dogs have been used as a protective measure against mountain lion attacks on livestock.
Running away and playing dead are considered ineffective strategies because running triggers the chase mode of the mountain lion and playing dead or standing very still makes the victim appear like an easy target. Historically, humans who have survived attacks have made themselves large and loud. Travis Kaufman notably strangled an attacking mountain lion to death when the animal refused to back down. There are concerns that mountain lion attacks are on the rise due to various factors. Hikers should remain vigilant and consider how they would defend themselves as well as their canine and human companions in the event of a mountain lion attack. Preparedness can be prevention.
Sneaker Waves: What Are They and Why Should We Care?
Pharibe Pope, MS-II
University of Maryland School of Medicine
Written on June 14, 2022 | Volume 39, Issue 2
On the afternoon of Sunday, May 29, two hikers were swept to sea by waves roughly a mile north of the Black Sands Beach trailhead in Northern California's Lost Coast.
The Shelter Cove Fire Department deployed a team of two ocean rescue units and two beach rescue units to the scene where the hikers were last spotted. After one hiker was reportedly dragged into the water by an unexpected surge of waves, a second hiker attempted to swim out to save them while other members of the party called for help. Both hikers who entered the water were found 50-100 yards offshore: one actively treading water and the other face down, declared dead on the scene by rescuers. The conscious hiker was transported by boat and air ambulance to the nearest medical center for further evaluation.
Sneaker waves are sets of waves that can suddenly and forcefully surge more than 150 feet further up the beach than expected. Beachgoers can be caught off guard because the surf may initially look calm and they are far from the foam line. However, true to their name, sneaker waves can appear at any time, without warning. Traveling at high velocities, these waves are potentially deadly, with the risks of propelling logs and heavy debris into beachgoers or even pulling them out to sea.
The steep, tree-lined coastlines of Northern California, Oregon, and Washington are more likely to cause sneaker waves than flat, broad beaches like those of Southern California. In fact, Lt. Micaela Crabtree of the 13th Coast Guard District declared sneaker waves one of the largest weather threats to beachgoers in the Pacific Northwest. Steep beaches lack the ability to slow down high-velocity waves. Log roll debris on the shoreline combined with frigid water temperatures and strong rip currents pose a threat to individuals caught in sneaker waves. If hit by a sneaker wave, individuals may experience large volumes of sand, water, and gravel deposited in their clothes, further preventing them from escaping forceful currents.
The National Oceanic and Atmospheric Administration (NOAA) recommends several steps to avoid sneaker waves:
- Arrive knowing the local weather, surf, and tide forecast
- Never turn your back on the ocean
- Watch the waves from higher ground for 20 minutes before moving closer to the water, continuing to watch until you leave
In addition, the Oregon Discovery team recommends the following:
- Avoid jetty rocks, mainly during high tide and storms, and when a Beach Hazards Statement is in effect
-
Supervise your children and pets and stay away from the surf zone
-
Do not turn your back on the ocean and avoid logs, rocks, and debris
-
Watch out if an incoming wave swells higher than the previous one
-
If you see the high wave is coming, move to high ground
-
Carry a walking stick, umbrella, or another straight object when you walk on the beach
-
If the sneaker wave comes up, do not panic, plant your walking stick into the sand as deep as possible and hang on until the wave passes
-
If you are caught by the sneaker wave, swim parallel to the shore until you are out of the wave, then swim toward shore
Beyond the Pacific Northwest, sneaker waves have been reported on the coasts of British Columbia, southern Iceland, western Australia, and Tasmania. Increasing awareness around sneaker wave safety may help to minimize fatal encounters in the future.

Sneaker waves along the Pacific Northwest
Source: WIN-Initiative - Getty Images
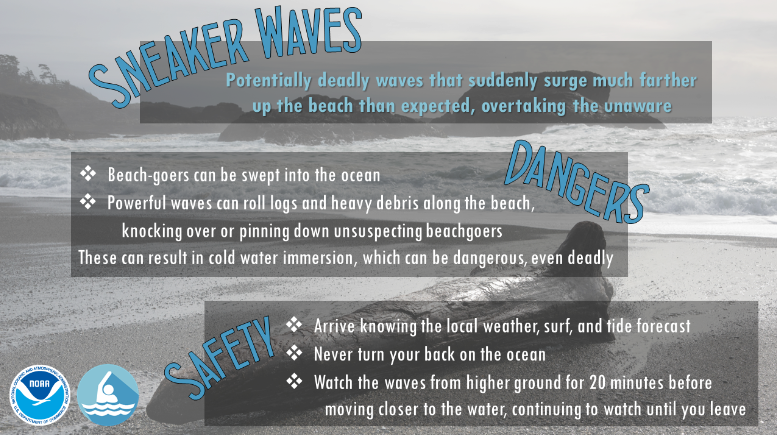
Sneaker wave informatic
Source: Weather.gov
Improvised Tourniquet Saves Climber Dalton Snow After Climbing Accident
Elaine Yu, DO, MS, FAWM
Kings County Hospital / SUNY Downstate Medical Center, Emergency Department
Written on May 10, 2022 | Volume 39, Issue 2
Dalton Freeman Snow, 29, was injured on April 12 while climbing to rig a highline near Moab, UT. As described on his GoFundMe page, he dislodged a mini fridge-sized rock while climbing over it, which nearly tore off his arm as he fell over 30 feet. He was roped up at the time and his belayer caught his fall six feet above the ground. However, his body sustained a vertical impact against the slab wall which broke his pelvis, five ribs, collar bone, and scapula.
Dalton was climbing with two friends, Lorenzo DeMuro and James Xu, both Wilderness First Responders, who utilized their training to improvise a tourniquet from cordelette on his arm and keep him warm while alerting search and rescue teams to extract him. Snow recalls his hand dangling off my wrist and the blood pouring out, which subsided after his friends placed a tourniquet, at which point he knew, I'm going to pull through. When rescue crews arrived, his climbing partners further helped place gear along the rock to aid rescue crews as they hauled him up to an area where he could then be airlifted to the hospital. He was first taken to a trauma center in Grand Junction, Colorado, where he was initially stabilized and further transferred to Denver for further surgical intervention, where he is now recovering.

Lorenzo DeMuro (left) with Dalton Freeman Snow while awaiting rescue.
Source: Climbing.com
DeMuro describes the fall as a freak accident, as the route was well within Snow's climbing ability. Instead, it was loose rock on the rarely-climbed route that caused the accident. Although Snow had tested the block by trying to wiggle it, it only came loose when he put his entire weight on it. Kiley Hartigan, a close friend of Snow, credits Xu and DeMuro for saving Snow's life with their improvised tourniquet. DeMuro noted that medical training is the lightest form of gear, and emergency training is important when accidents occur.
In a 2015 review in the Journal of Trauma and Acute Care Surgery, the authors concluded that certain improvised tourniquet designs such as the windlass type, can be as effective as, if not better than, commercially available tourniquets at controlling arterial blood flow in a limb. Windlass tourniquets are created by using a strong stick or rod-shaped object (the windlass) in conjunction with a band tied around a hemorrhaging limb. The windlass is secured to the band and then twisted continuously in either a clockwise or counterclockwise direction to tighten the band using mechanical advantage and apply enough pressure to slow or stop arterial flow to the distal extremity.
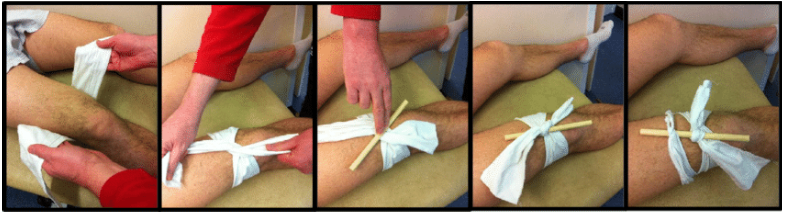
Source: Stewart et al. Improvised Tourniquets: Obsolete or obligatory? Journal of Trauma and Acute Care Surgery. January 2015. 78(1):178-183.
In a comparison study between chopsticks, pencils, and craft sticks, chopsticks were the least likely to break during construction of an improvised tourniquet on a simulated manikin. A study of first-year medical students found that 38% were unable to control hemorrhage after being given a windlass tourniquet with enclosed instructions, highlighting the importance of tourniquet training. Prehospital tourniquets are applied by both EMS and non-EMS personnel with equal rates of proper application.
46-Year-Old Man Dies During Iron Man 70.3 in Galveston, Texas
Sarah Spelsberg PA-C, FAWM, MS-IV | Sara Filmalter MD, FAWM/DiDMM Candidate
Written on April 8, 2022 | Volume 39, Issue 2

Daniel Winkler, a 46-year-old triathlete from Arlington, Massachusetts, died April 3 after being found underwater during the swim portion of the Memorial Hermann 70.3 Ironman race in Galveston, Texas. The race includes a 1.2-mile swim, a 56-mile bicycle ride, and a 13.1-mile run. Winkler is survived by his wife Regan, two daughters, family, and friends.
Winkler was discovered motionless amongst other swimmers and safety kayakers. He was given CPR on scene by first responders. He was transported to a nearby hospital by ambulance and efforts to revive him continued for over an hour when he was ultimately pronounced dead.
John Florence, chief investigator with the Galveston county medical examiner's office, reported that the cause of death was pending but didn't appear to be drowning, according to The Globe. The Galveston county medical examiner continues to investigate the cause of death.
The risk of sudden death in endurance athletes is low but not insubstantial. Marathon deaths are estimated at 0.67 per 100,000. The incidence of death during US triathlons in one study is reported at 1.74 per 100,000. Most of the deaths during a triathlon occur during the swim portion of the event and more often in men. There are a few proposed causes of the sudden deaths reported during the triathlon swim leg.
One proposed mechanism is immersion pulmonary edema (IPE). This is supported by greater than background incidence of left ventricular hypertrophy found in deceased triathletes in one study. Immersion pulmonary edema is more likely to occur during cold water immersion and exercise which can lead to an increase in pulmonary capillary pressure. Eventual pulmonary capillary stress failure causes flooding of alveolar spaces and subsequent pulmonary edema.
Another proposed mechanism for the swim deaths is antagonism between parasympathetic-induced bradycardia from facial immersion and diving reflex and sympathetic adrenaline from the race start. The competition between the two can cause QT prolongation, torsades de pointes, and eventually ventricular fibrillation.
Some triathlon medicine experts have proposed screening questionnaires and modifications to races, including minimum water temperatures, the elimination of the mass start, as well as adequate spacing of rescue teams and boats to try to decrease the risks to triathlon participants. While the risk of death in triathlons is extremely low, the implication of being one of the few is not insignificant, and this has recently left a woman without her husband and two young girls without their father.
Equipment Failure Leads to Climbers Death in Joshua Tree
Seth Thomas, MS-III
University of Cincinnati College of Medicine
Written on April 6, 2022 | Volume 39, Issue 2
On the weekend of March 26, Tina Fiori set out for a day of climbing near the Wailing Sax area of Joshua Tree National Park with two companions. One of the climbers was celebrating a birthday and over 2,000 ascents in Joshua Tree. Tina was known for developing dozens of routes in southern California. They were not a novice group of climbers. The trio finished their day by top roping on a climb named “Turkey Terror.”
Top roping involves creating a redundant anchor at the top of a climb, often utilizing two permanent bolts. A belayer is stationed on the ground and the climber is continuously underneath the anchor as they climb. This system has a lower potential for lengthy falls and is regarded as one of the safest ways to climb. At the end of the day, Fiori climbed “Turkey Terror” to retrieve the gear composing the anchor and went off belay: she would rappel to the ground utilizing a piece of tat.

The Wailing Sax Wall at Joshua Tree National Park. Photo Credit: Bill Odenthall
Climbing tat is a term that refers to pieces of webbing, cord, or climbing rope that are permanently tied around a structure such as a boulder, tree, or section of the cliff face to provide a way for climbers to descend. They are commonly found in alpine settings or rock climbing areas.
As Fiori weighed the climbing tat at the top of Turkey Terror, it failed. She fell the approximately 60 feet to the base of the cliff. First responders found her dead at the scene.

An example of a rappel utilizing a piece of tat.
Photo credit: https://www.straightupadventures.co.uk/abseil-anchors
Similar incidents have occurred in the past, including an example of a party of three completing several rappels near Juneau, Alaska. The first climber set up a rappel utilizing a piece of tat and descended safely. The second climber to rappel broke the tat, which was at least a year old, and fell to his death.
Rappelling is one of the more dangerous events encountered in a day of climbing. Compiled data from 30 years of climbing accidents tells us exactly how dangerous it is. Of all the different approaches to climbing, traditional (or “trad”) climbing makes up a significant portion of climbing accidents at 63%. Rappelling errors are one of the more common causes of incidents at 12%. Inadequate protection (49%) and failure to wear a helmet (14%) are also common culprits. Rappel errors tend to be more serious with a 39% fatality rate.
There are several factors that can explain why descending is often more dangerous than ascending rock faces. Fatigue is a significant contributor, as descending typically occurs at the end of a climb. Climbers are more likely to make mistakes or overlook small details when fatigued. Descending typically also involves transitioning from one system of protection (the belayer) to another (a rappelling device), a transition that can require significant technical coordination.
In this incident, the equipment was the point of failure. It is challenging for climbers at all levels of experience to accurately judge how long a piece of tat may have been left in place. Replacing in situ gear is the most conservative approach to staying safe when descending with gear in place, even if it may come at a slight cost of additional equipment. Slings and other pieces of climbing gear are all replaceable. The damage caused by a fall can be irreparable.
Avalanche Risk: Not Just Something for Skiers, Snowboarders, and Alpinists to Think About
Amanda Michelle Ritchie, MD, PGY-I
Louisiana State University Health Sciences Center
Written on March 8, 2022 | Volume 39, Issue 1
There have been 845 witnessed avalanche slides in Colorado so far this season, 303 of which were triggered by humans. Backcountry skiers, snowboarders, and alpinists are often the first that come to mind when thinking about which groups are most at risk for avalanches. However, snowshoers, snowmobiles, and hikers are also at risk. While the latter groups may not travel in all of the same high-risk areas, there are still risks of travelling through avalanche tracks or run-off zone.
On February 25, a group of four hikers and two dogs were out snowshoeing in the lower portion of Yule Creek in Colorado. An avalanche 50 feet wide was triggered when three of the people and two dogs headed towards a mid-slope road, pushing them onto the sides of a steep gully. Two people were partially buried but were able to dig themselves out. The third person and both dogs were completely buried and declared dead on scene.
On January 8, two people and their dog were snowshoeing on Hoosier Pass near North Star Mountain in Colorado. The initial search for the pair commenced on January 9 after they failed to meet up with friends for a planned post-hike get-together. Police found their vehicle at the top of Hoosier Pass and a Flight for Life survey revealed a large amount of avalanche debris that was believed to be the cause of the missing couple. The avalanche ran 250 vertical feet, 10 feet deep, and 400 feet wide. They were not carrying avalanche transceivers.
The Colorado Avalanche Information Center compiles data of accidents and fatalities throughout the years. To date this season, there have been eleven avalanche fatalities: three skiers, five snowmobilers, and three snowshoers/hikers. Of those eleven deaths, four of them occurred in Colorado. Of the 267 avalanche fatalities in the past ten years, snowshoers/climbers/hikers have totaled 46 (17% of deaths) and snowmobilers 80 (30% of deaths), together totalling 47% of all avalanche deaths reinforcing the importance of avalanche awareness for all those recreating. in steep and snowy terrain.
The WMS Avalanche and Snow Burial Practice Guidelines were published to help guide care for these patients. There are multiple factors involved in the morbidity and mortality of avalanche victims, including burial duration and depth, airway patency, volume of air pocket, and associated traumatic injuries.
The WMS guidelines include a flow chart for the assessment of patients who were fully buried after extrication:
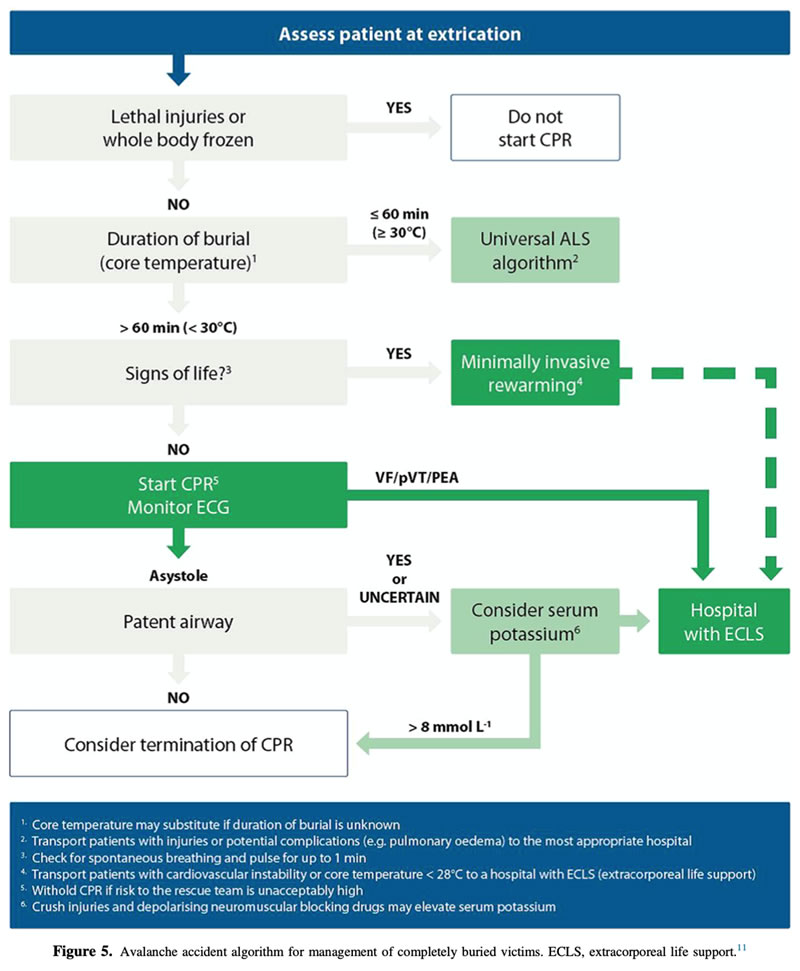
Cause of death by asphyxia is estimated at 75% of cases, trauma at 25%, and very few related solely due to hypothermia.
Asphyxia
- Time to extrication is critical in survival. Extrication within 15 minutes has been shown to have more favorable rates of survival (up to 90% in one study) but significantly drops (30% or less) if extrication occurs around 30 minutes after burial.
- Death occurs by three mechanisms:
- Snow can physically block the airway hypoxia results in less than 10 minutes, with acute asphyxiation in 30-60 minutes.
- Formation of an ice mask occurs when exhaled water vapor freezes on the snow creating an ice wall barrier impeding effective gas exchange.
- Rebreathing expired air causes oxygen deprivation duration of survival is directly proportional to the size of the air-pocket at burial. A longer duration of burial results in a progressive decrease in fraction of inspired oxygen and increase in fraction of inspired carbon dioxide.
- An additional factor is the weight and compression of snow preventing adequate inspiratory volume and impairing respiration.
Trauma
- Accounts for 25% of burial deaths in avalanches caused by recreational sports, however, the percentage climbs rapidly with larger catastrophic avalanches such as the 2014 Khumbu Icefall on Mount Everest and the large avalanches occurring during the 2015 Nepal earthquake.
- Injuries vary and can include life-threatening trauma to the head, spine, chest, or extremities caused by blunt trauma with trees, ice, or rocks.
Hypothermia
- Hypothermia is a complicating factor in many burials but is not often a primary cause of death as asphyxia often occurs prior to fatality from hypothermia.
Italian Alpinist Korra Pesce Dies After Avalanche Leaves Him Paralyzed on Cerro Torre
Elaine Yu, DO, MS, FAWM
Kings County Hospital / SUNY Downstate Medical Center, Emergency Department
Written on February 8, 2022 | Volume 39, Issue 1
On January 28, 41-year-old Italian alpinist and mountain guide Corrado “Korra” Pesce and 36-year-old Argentinian alpinist and mountain guide Tomas “Tommy” Roy Aguilo were injured after a rime-ice mushroom broke off during their nighttime descent of Cerro Torre, a technically difficult mountain in the Southern Patagonia Ice Field. They had summitted the mountain by a new route just hours before, a multi-year dream for the pair of alpinists. The resulting avalanche of ice and rock swept away most of their gear and left Korra paralyzed and Tommy injured but mobile. Tommy was able to continue to rappel and recover their inReach, a satellite messenger device, and call for help.
Climbers in the Niponino base camp, more than a two-hour hike away, had seen an SOS signal and a team had gone up to investigate. Less than 24 hours later, an Italian team (Matteo Della Bordella, David Bacci, and Matteo De Zaicomo), who had last seen Korra and Tommy at the summit after also completing a separate new route, met up with rescuers at the base of the mountain and learned of the tragedy. Della Bordella used his drone to locate Tommy and prepared himself to climb up to him with German alpinist Thomas Huber, Swiss alpinist Roger Schaeli, and Argentinian Roberto “Indio” Treu from the rescue party.
The four climbers reached Tommy within a few hours and Treu and Huber descended with Tommy while Della Bordella and Schaeli waited in the cold and wind of an incoming storm until the last minute for any sign of Korra, finally giving up when Della Bordella became delirious. Once off the wall, Tommy was carried down the glacier at the base of Cerro Torre to a helicopter which flew him to a hospital where he was found to have broken a clavicle and multiple ribs with associated pneumothorax. He is expected to recover from his physical injuries.

Cerro Torre. Tommy was able to rappel to the triangular snowfield partway down before meeting his rescuers. Source: Roger Schaeli / Alpinist.com
Days later, Korra’s body was located by drone. According to the El Chalten Alpine Rescue Center, Korra “can no longer be alive” as “death from hypothermia occurs within two hours” in those conditions.
Hypothermia occurs when your body is no longer able to maintain its core temperature. Environmental factors, such as temperature, windchill, and humidity exposure, can accelerate heat loss from the body. The body, in response, attempts to counter heat loss via peripheral vasoconstriction, shivering, and cold diuresis. As the body’s temperature continues to drop, brain activity decreases and manifests as confusion, lethargy, and eventually becoming comatose. At the same time, the heart may develop abnormal conduction triggered by the slightest movement, which manifests as dysrhythmias that can lead to cardiac arrest.
According to the WMS Practice Guidelines for Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: hypothermia is defined as mild (32-35°C), moderate (28-32°C), and severe (<28°C). However, measuring core temperature is not always possible in the field. Therefore, patients can be assessed based on their mentation and ability to move (Figure 1). Patients who are able to shiver should be insulated from the environment to maintain heat (Grade 1A). Rewarming can start in the field with active heat sources in conjunction with vapor barriers and insulation (Grade 1B). Body-to-body rewarming can be used if it does not delay evacuation (Grade 1B). During evacuation, hypothermic patients should be kept horizontal and avoid any disturbance that might precipitate ventricular fibrillation (Grade 1B). Despite the adage “nobody is dead until they are warm and dead,” a patient with obvious signs of fatal injuries or a chest too rigid to do compressions should not be resuscitated (Grade 1A).
Whenever attempting a remote or technical objective, self-rescue should always be a consideration as help may be hours or days away. Climbers and mountaineers should have knowledge of self-rescue techniques as well as ways to help an injured partner down the mountain. If unable to advance from your position, gear for a bivouac (bivy), or temporary encampment, should be available to protect from the elements. From there, you can call for help with a satellite communicator or personal locator beacon (PLB).
PLBs are used in an emergency and send a signal to a satellite network that then sends your information and location to the closest rescue authorities. You cannot send or receive messages, and some only send out your location once so if you move the rescue personnel will only know your last location. In contrast, satellite communicators allow you to personalize a message and send it with your location. Some, like the inReach used by Korra and Tommy, have the ability for two-way messaging so that rescuers can send you updates and instructions to assist with your evacuation and view your location in real-time.
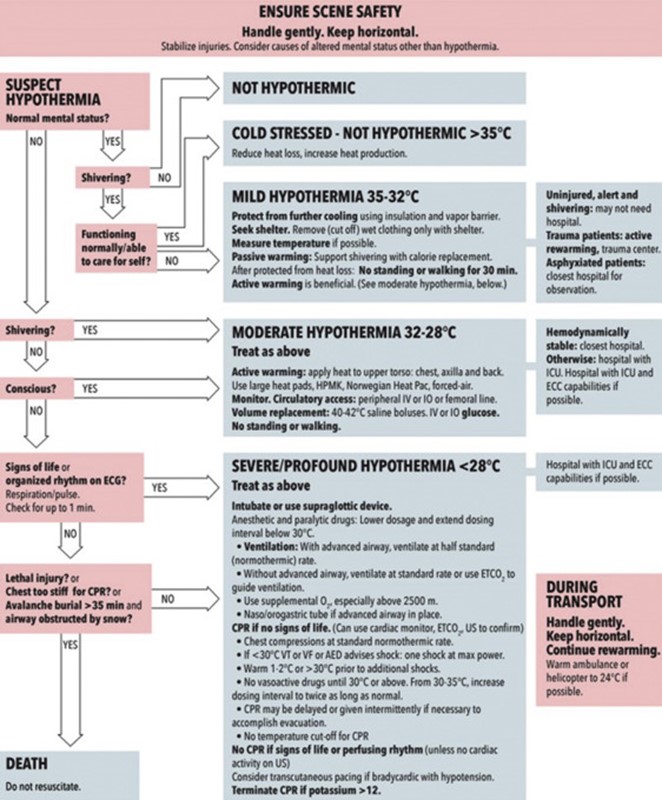
Figure 1: Recommendations for out-of-hospital evaluation and treatment of accidental hypothermia. Source: Wilderness Medical Society.
Ten dead after rock face collapses on boats in Brazil Furnas Reservoir.
David Gordon, W-EMT, EDAC, MS-I
Sidney Kimmel Medical College, Thomas Jefferson University
Written on January 10, 2022 | Volume 39, Issue 1

(video screenshot, Credit: Record TV Minas, Twitter)
Brazil’s Furnas Reservoir in the state of Minas Gerais has become a popular boating destination due to its 20-meter-tall canyons offering scenic waterfalls flowing into the lake, especially after recent heavy rainfall. In one section of the canyon, near the town of Capitlio, approximately one hundred recreational boaters were watching the falls on January 9.
While the boaters were on the water, reports suggest the waterfall flow notably increased. Some of the boaters observed nearby rocks tumbling down the cliffside into the lake and attempted to leave the area. Seconds later, a fissure suddenly enlarged on the cliff and a column of rock collapsed directly onto at least three boats.
Two of the boats sank immediately. The collapse was recorded in a shocking video, initially posted to social media. As of January 10, ten people have been reported dead in addition to at least thirty more injured with nine requiring hospitalization.
What may have caused the cliff to collapse so suddenly? Heavy December and January summer rains in Southeast Brazil have increased floods in Minas Gerais, likely also prompting water infiltrating into the sedimentary rocks of the canyon. This infiltration of a fissure in addition to centuries of undercutting erosion at the base of the cliff and progressive instability of saturated soil could have contributed to the cliff’s sudden collapse.
The Minas Gerais State Fire Department initiated a search and rescue operation following the collapse, including dive rescue personnel and aircraft. The Brazilian Navy has begun investigations on the event.
While erosion and canyon cliff collapse are natural phenomena, the increase in tourism to the area may lead to more people coming closer to potentially unstable rock faces. Up to 30,000 people have been known to visit Capitlio (population 8,000) on a single weekend, with canyon boat tours being a popular activity.
With a rescue following such a harrowing cliff collapse, rescuers would have needed to determine the integrity of the remaining cliff to ensure the rescue and recovery attempt would not be compromised. Some geology experts have noted that authorities should begin regulating access to the area with public safety measures, especially in the rainy season, to minimize people entering potentially unstable terrain. Future guidance on safe navigational areas near the cliffs, including a minimum required distance between vessels and the cliff walls, could increase the margin of safety in the future.
Rescue on the Sandia Peak Tramway outside of Albuquerque, NM
J. Austin Martin, MS, AWLS, WFR, OMS-II
West Virginia School of Osteopathic Medicine
Written on January 7, 2022 | Volume 39, Issue 1

Credit: AP / Roberto E. Rosales
On New Year’s Day, twenty-one people were rescued from two tram cars on Sandia Peak Tramway outside of Albuquerque, NM after a nearly 15-hour ordeal. The majority of the passengers in the stuck tram cars were employees of Ten 3, a restaurant at the top of the Tramway. After their New Year’s Eve shifts were over the employees began their descent in two tram cars around 8:45 p.m., a descent which typically takes about fifteen minutes.
According to the tramway’s general manager, Michael Donovan, high moisture in the air and low temperatures led to ice accumulation on one of the tram’s cables, which forced the tram cars to a halt. Bernalillo County Fire Department was called around 2:00 a.m. to assist in rescue efforts. As weather conditions failed to improve and the likelihood of allowing the cars to descend decreased, the decision was made to rescue the passengers directly from the tram cars. Meanwhile, the occupants huddled to stay warm and utilized the emergency food, water, and space blankets that were supplied on the tram cars.
By Saturday morning, rescuers had hiked up to the tram tower nearest the stuck cars, ascended the tower, traversed across a cable, and delivered additional blankets and other supplies to the trapped occupants. Then, in the early afternoon, a rappel was rigged from the first tram car which contained 20 of the 21 passengers; this allowed rescuers to assist the passengers in descending approximately 85 feet to the ground. They were then moved to a small landing zone nearby where they were evacuated by helicopter in small groups.
According to Bernalillo County Undersheriff Karry Koren, the rescue was prolonged as there were intermittent periods of inclement weather which produced very low visibility; this meant that the helicopter could only fly sporadically during short periods of improved visibility. All 21 passengers were assessed medically after being flown off of the mountain and were alive without serious injuries.
While incidents on the Sandia Peak Tramway are rare, they do occur. In August 2020, two cars were stuck for about four hours due to a “mechanical problem,” which was then resolved. All occupants were uninjured in the event. In June 1973, 32 passengers were stuck for over 24 hours in a tram car suspended 650 feet in the air. At that time the Sandia Peak Tramway was the world’s longest aerial tram.
Incidents like this occur worldwide. Some of the more recent incidents have involved tram cars in the French Alps and Italian Alps. Unfortunately, these incidents sometimes result in fatalities. In the Czech Republic, one person died and others were injured after a tram car detached from the cable in October 2021. In Italy last May, 13 people died after a cable car plummeted to the ground after a cable broke.
Trams (also known as gondolas, cable cars, or aerial lifts) serve as an important form of transportation in some mountain regions, particularly near ski areas. It is important that they be closely regulated and meticulously maintained to ensure that incidents such as these are avoided. Furthermore, it is critical that local officials including SAR teams undergo regular training and perform rescue scenarios in order to be ready for events such as these.
New study looks at CPR effectiveness at altitude
Robert J. McMickle, MD, PGY-III
Harbor-UCLA Emergency Medicine
Written on December 20, 2021 | Volume 39, Issue 1
When helicopter emergency medical service (HEMS) providers were put into simulated high altitude environments up to 5000 meters, the quality of their chest compressions decreased significantly over time, according to a new December 2021 study in the Journal of the American Heart Association.
Even more, participants did not recognize the ongoing loss in quality of cardiopulmonary resuscitation (CPR) over time, with loss in quality occurring as soon as 60 to 90 seconds after starting. Study authors Vgele et al. reported that, “there is a significant risk that the depth of [chest compressions] can drop below the recommended 50mm already before two minutes.”
Forty-eight helicopter emergency service personnel from Germany, Italy, Austria, and Switzerland were exposed to altitudes of 200, 3000, and 5000 meters in the extreme climate simulation center, the terraXcube, at the Eurac Research Institute in Bolzano, Italy.
Participants “ascended” at a rate of 4 m/s (a typical helicopter ascent rate) to one of the three pre-selected altitudes (the study center utilized an oscillating ascent/descent profile to mimic pressure changes on participant’s eardrums). They then performed CPR on standardized mannequins connected to an electronic tablet for recording while having their heart rates, respiratory rates, and pulse oxygenation recorded. Afterwards, participants were then asked to rate their performance and effort.
While groups at all altitudes demonstrated at least some degree of decline in chest compression rate, depth, and number of effective compressions, the detriments occurred sooner at higher altitudes. The effect was more pronounced in female providers and providers under 70 kg, though the authors note the study was not designed to assess differences in sex.
Perhaps not surprisingly, twenty minutes after the initial ascent, participant’s pulse oximeter readings were significantly lower in the higher altitude groups both before and after compressions (approximately 78% at 5,000 meters vs 96-98% at 200 meters), suggesting a baseline hypoxia contributed to the progressive decline in performance.
“Our findings highlight the need to raise awareness in providers on a potential decline of their [chest compression] performance over time at altitude. It also raises the question of whether the recommended two minute cycle should be applied to providers subject to rapid exposure to moderate and high altitudes such as HEMS personnel,” authors note, suggesting that more frequent changes in chest compressors may improve overall CPR quality.
At altitude, the combination of hypoxia, cold temperatures, and physical exertion increase the risk for sudden cardiac arrest, especially in older populations with underlying comorbidities such as hypertension or heart disease. Furthermore, cardiac arrest patients at high altitudes experiencing concurrent severe hypothermia may require much longer than normal CPR times.
High quality CPR remains the cornerstone of resuscitation in cardiac arrest patients and poor quality CPR is considered a preventable harm. Ongoing research into mechanical compression devices already utilized by EMS agencies and emergency departments across the world have yet to yield conclusive results, though there as has yet to be a comparative study of these devices in high-altitude environments.
“Mechanical CPR devices achieve similar resuscitation quality compared with high quality manual delivery of [chest compressions], and the availability of these devices might be especially relevant for management of cardiac arrest during HEMS operations at high altitude,” the study authors note.
They also add that the “advantages could be that mechanical CPR devices can deliver continuous compressions without degradation of quality even in prolonged resuscitation and without need for provider changeover, especially during transport and transfer, where manual [chest compressions] might not be feasible or possible at all.”
The authors note their study, though randomized, single-blinded, and placebo-controlled, did not replicate true environmental conditions for participants and external factors such as wind, snow, raised sympathetic activity and alertness may further impact results as well the effects of a more gradual ascent and acclimatization. Additional studies into environmental conditions as well as the use of supplemental oxygen in participants at altitude would help shed future light onto this critical ongoing field of research as more and more people take to the mountains for recreation.
Washington ski resort avalanche leads to death of 1 man, rescue of 5 others
Mary Rosegrant, DO, PGY-IV
UT Health Science Center - San Antonio
Written on December 15, 2021 | Volume 39, Issue 1
Crystal Mountain, Washington’s largest ski resort located 85 miles southeast of Seattle near Mount Rainier, saw an avalanche sweep through its outer boundaries around 10:50 a.m. on December 11 as a group of backcountry skiers were traveling uphill in a section known as Silver Basin. According to the Northwest Avalanche Center’s preliminary accident reports, four of the six members of the party had been partially or fully buried. With the help of two nearby witnesses, rescue efforts quickly ensued. Five of the trapped travelers were rescued alive, however one 60-year-old man was pronounced dead on the scene by authorities despite initial CPR efforts.

The group of experienced backcountry skiers had participated in the resort’s orientation regarding backcountry skiing, registered with ski patrol, and acquired uphill travel passes. Though the Silver Basin held warnings against skiing due to weather conditions, the skiers found themselves in the high-risk area after venturing into the Mount Baker-Snoqualmie National Forest, which abuts the resort.
The mountain range had seen heavy snowfall over the weekend, as much as 12 inches in a 24-hour period, and wind gusts up to 100mph led to closure of the resort’s Mt. Rainier Gondola. The forecast continues to call for consistent snowfall in the coming week, increasing the potential for additional avalanche activity.
Avalanche control and defense encompasses a wide range of group and individual efforts, including terrain assessment, zoning, mitigation strategies, and personal education and preparedness. Understanding these strategies at all levels can go a long way in helping to reduce the risk of being involved in an avalanche unexpectedly and can improve chances of survival if one is caught in a snow slide.
Preparedness/Safety Tips:
As outlined in a recent WMS Breaking News article (see November 14, 2021), it is important to understand the 3 main factors that lead to avalanches:
- Slope steeper than 30 degrees
- Stability of snowpack, which is influenced by recent and underlying snow quality, weather conditions, or recent avalanches
- Triggers, such as mechanical agitation (e.g., people, snowmobiles), new snow, and wind
Signs of unstable snowpack include:
- shooting cracks in the snow
- evidence of prior avalanche
- hollow feeling underfoot or “whumping” sounds
- weather changes, including heavy snow or rainfall in previous 24 hours or rapid temperature changes
Terrain, Zoning, and Risk:
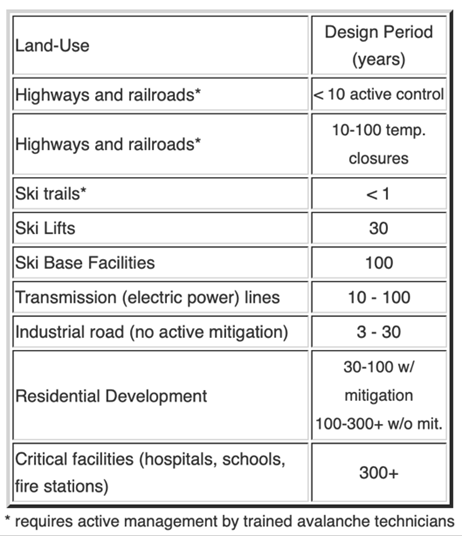
On a macro scale, structural engineers are involved in evaluating areas at risk for avalanche. This includes review of historical accounts of avalanches, slope steepness (highest risk at 30-50 degrees), and surveying of vegetation (e.g., evidence of tree damage and robustness of forestation). In areas that are avalanche-prone, zoning identifies areas of high, medium, and low risk of destruction in the event of avalanche flow. The following table outlines typically accepted avalanche return periods for different categories of publicly used roads, structures, facilities, and buildings.
Mitigation Strategies:
Avalanche mitigation techniques are divided into non-structural and structural methods. Non-structural approaches include land restrictions (passive) and artificial triggering (active). Artificial triggering intentionally disrupting unstable snowpack can be accomplished by simply walking over small unstable areas or by detonation of explosives. There are multiple strategies for deployment of explosives; this video from a planned Crystal Mountain Resort explosion in 2014 shows the sometimes unintentional effects of artificial triggering. Structural mitigation strategies include snow dams, sheds, nets, and strengthening of existing structures to withstand impact. Social interventions (e.g., avalanche education courses and outreach programs) are also implemented to help modify human behavior as a means to reduce avalanche risks.

Proper equipment:
Three essential pieces of equipment recommended for backcountry skiers include:
-Transceiver
-Snow Probe
-Shovel
Education:
In the event that one finds themselves involved in an avalanche or participating in a search and rescue situation, avalanche-specific training is essential and can improve the chances of successfully finding and recovering buried victims. Backcountry Access provides multiple videos reviewing different aspects of avalanche rescue. Additionally, the American Avalanche Association and the American Institute for Avalanche Research are great resources for all things avalanche.
Coast Guard helicopter rescue from partially submerged vehicle above Niagara Falls.
Seth Thomas, MS-III
University of Cincinnati College of Medicine
Written on Dec 8, 2021 | Volume 39, Issue 1
Niagara Falls is the largest waterfall in North America, with water spilling down at a rate of up to six million cubic feet per minute. It has also been the site of many daring rescues, as seen in early December.
A driver in a black sedan entered the raging waters of the Niagara River just before noon on December 8. The vehicle was spotted floating past a pedestrian bridge towards the brink of the falls and 911 calls began to flood in. The car halted a mere 50 yards from the top of the 180-foot tall cascade with powerful waters partially submerging the sedan.

Photo Credit: Jeffrey Barnes, Associated Press.
Petty Officer 2nd Class Derrian Duryea descends to the partially submerged vehicle.
Local fire crews, state police, and state park police responded to the scene. Initial attempts to perform a roped rescue were led by police and fire rescue teams. Ultimately, roped rescue was unsuccessful as the swiftwater teams were unable to secure enough anchors to safely perform a rescue. The U.S. Coast Guard mobilized a helicopter crew from Detroit to perform an air rescue.
While air rescue efforts were being organized, a state police drone was employed to gather information about the car and its driver. The drone was able to successfully visualize the license plate number and monitor the passenger while rescue attempts were being organized. No movement was seen from the passenger inside the car. The New York Power Authority lowered the upstream water level of the river in order to prevent the fast-flowing water from dislodging the car and to ease the extrication once a rescuer was in position.
A U.S. Coast Guard MH-65 Dolphin arrived on scene at approximately 1:55 p.m. The crew consisted of pilot Lt. Chris Monacelli, flight mechanic Jon Finnerty, and Petty Officer 2nd Class Derrian Duryea. Duryea, equipped with extrication tools, was quickly lowered down to the car. He was able to access the vehicle without the need for forced entry and secured the sole passenger for airlift to the riverbank, where EMS personnel were waiting. The passenger, a local woman in her 60s, was confirmed dead at 2:15 p.m. Investigators currently believe that the car may have entered the water intentionally. The cause of death is still under investigation.
Swiftwater Rescue
The rescue of individuals who have become entrapped in fast flowing waters can be a complicated task that requires both specialized training and the ability to improvise. The breadth and depth of swiftwater rescue cannot be covered here; however, some important elements are introduced below.
- Throw Bags
In the case of a conscious and cooperative victim who can hold onto a line, the throw bag is the fastest option that can have a high success rate. Complicating factors include distance between the victim and shore, water flow, debris in the water, and strainers.
- Tensioned Diagonal System
In the case of an unconscious victim or more complex rescue, a tensioned diagonal system can be a fast and adaptable rescue technique. Two anchors on opposing sides of the river are used to create a line that intersects the location of the victim. Individual rescuers or whitewater rafts can use the line for support (as seen below) to ferry across to reach the victim.

Photo Credit: swiftwaterrescue.com
A tensioned diagonal line allowing a rescuer to safely move downstream in Yosemite National Park.
- Z-Drags
A Z-drag is a quick shoreline pulley system that gives a 3:1 mechanical advantage when trying to haul a pinned boat or victim against a strong current (named after the Z-shape created by the hauling rope, see below). To create a Z-drag system, a rope is secured to the object you intend to haul and a strong riverside anchor.
A progress capturing system, such as a prusik knot, is essential as well as several rescuers to set-up, haul, and operate the system.
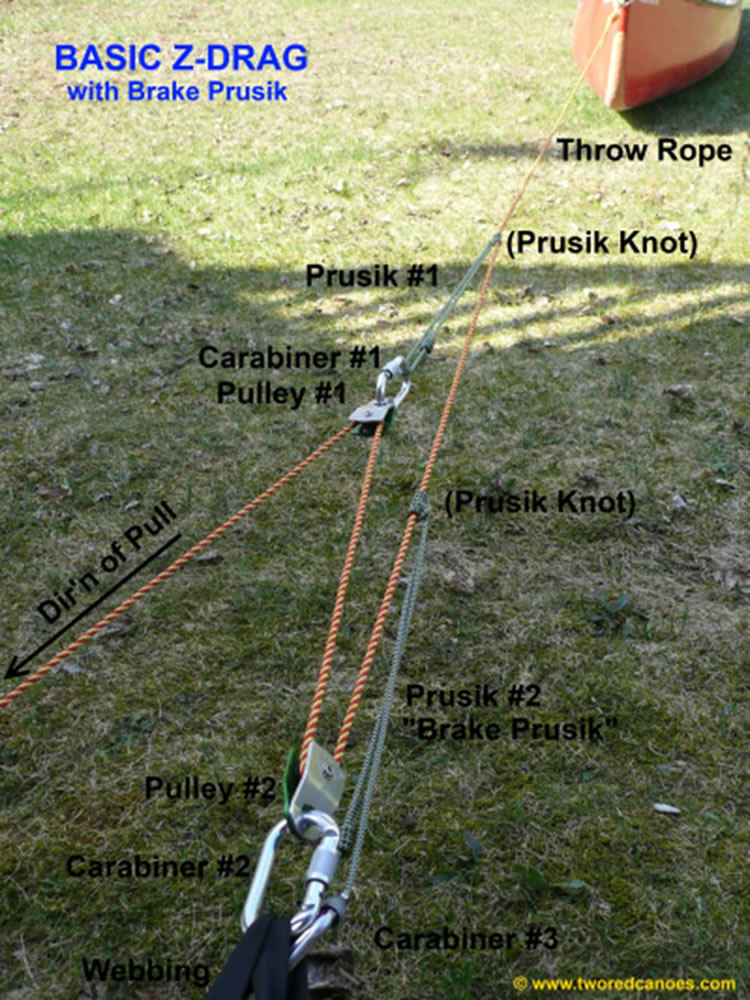
Photo Credit: tworedcanoes.com
An example of a Z-Drag with a progress capturing “brake Prusik” in place on the anchor.
Possible Suspension Syndrome in a Zion Canyoneering Accident
Brennan Enright, MS-III
University of Arizona College of Medicine Phoenix
Written on December 2, 2021 | Volume 39, Issue 1
On Sunday, November 28, a 31 year-old man, Andrew Arvig, died and two others were rescued in a canyoneering accident in Zion National Park. The group was canyoneering in Heaps Canyon, often undertaken as a one- to two-day technical canyoneering trip with numerous swims, potholes, and rappels through a narrow slot canyon. The final descent of the route involves a 145-foot rappel onto a small ledge followed by a second 280-foot rappel to the ground below to a place known as Upper Emerald Pools. In the accident, Arvig rappelled about 20 feet past the ledge where he was stuck free hanging in his harness from the rope. The other two members in his group used their tag line to rappel to the ledge. Arvig was unable to ascend back up to the ledge, so the group made a call for a rescue.
The rescue operation, helmed by the Zion Technical Search and Rescue Team, included over thirty rescuers and two helicopters from the surrounding region. Arvig was eventually lowered to the ground where he was pronounced dead by a doctor on scene. The cause of death is currently still under investigation. The other two canyoneers were able to descend to the ground safely.
Though the cause of death is currently not established, this tragedy is not the first description of death without an obvious cause seen in individuals suspended from a rope. This phenomenon, termed suspension syndrome, was first mentioned at the 2nd International Conference of Mountain Rescue Doctors in Innsbruck, Austria in 1972. Since then, descriptions of suspension syndrome have detailed climbers and cavers dying while suspended on a rope with no signs of trauma and time to death that was too rapid to be hypothermia. Several reports described individuals dying immediately following rescue and some detailed rhabdomyolysis following prolonged suspension.
The syndrome is not thought to be due to a solitary process and is not completely understood. Initial theories postulated that passive hanging from a harness led to venous trapping in the legs which led to reduced preload and subsequent syncope, muscle relaxation, and further worsening of leg compression, venous pooling, and poor vital organ perfusion. Some also postulated that relief of this pooling then led to cardiac overload and death upon rescue. This theory caused rescue organizations to recommend against supine positioning in a suspension victim following rescue. Follow-up studies have shown that lower extremity venous pooling did in fact happen in suspension from a harness, but degree of pooling was not associated with occurrence of syncope and echocardiograms did not show cardiac overload upon relief of suspension.
Another study provided further clarity by measuring venous pooling and the associated hemodynamic response in twenty participants hanging from a harness. They found that venous pooling occurred in all participants, but degree of pooling was not associated with changes in heart rate, blood pressure, or syncope. Instead, a drop in heart rate and blood pressure was seen in those experiencing syncope, suggesting a vagal response, not a lack of preload, as the cause.
On the ground, the syncopal response generally accomplishes its goal: flatten the person out to restore perfusion to vital organs. On a rope, however, syncope leads the person to lean backwards, arching their back with the legs still low, and the hips as the highest point. This position can further compromise venous return, worsening perfusion of vital organs which can be fatal.
Some have recommended prevention of suspension syndrome by preventing the initial syncopal episode. Individuals who are suspended should aim to continually move their legs to maintain venous return, elevate the legs if at all possible, utilize foot slings to alleviate stress on the body, and have the means to escape a suspension quickly if at all possible. If someone who is suspended loses consciousness, it should be treated as a medical emergency and that individual needs to be lowered as quickly as possible. As there is no evidence of cardiac overload upon relief of suspension and the syncope is thought to be primarily a vagal response, patients should be treated similarly to cases of vasovagal syncope and be placed in a supine position immediately upon rescue.
Canine Search and Rescue: Climbers Rescue Dog from Mexico Highest Peak
Heather S. Herman, MS-I
University of Miami Miller School of Medicine
Written on December 2, 2021

Credit: Hilario “Layo†Aguilar, Facebook
Canelo’s story first went viral on social media with the photos depicting him living for a month atop an inactive volcano in Mexico. At 5,636 meters, Pico de Orizaba is the highest peak in Mexico and third highest peak in North America after Denali and Mount Logan. However, Canelo is no seasoned mountaineer: he is a young dog who wandered up the volcano, likely following climbers with food. Social media followers clamored for his rescue, but climbers who spotted him said it would be too dangerous to bring him back down.
Local climber, Hilario “Layo” Aguilar, then decided to lead a group of mountaineers with the Mexican Alpine Club to the summit in search of “El Famoso Canelo”. The group coaxed the defensive pup into one of their backpacks and the team switched off carrying him down the mountain. Canelo had survived freezing temperatures and snow during his month atop the volcano. When he was finally rescued, he showed signs of malnutrition and a paw was injured and bleeding. Â Layo shared his account of the rescue on Facebook, describing their dangerous descent in difficult conditions. Upon his return, he was taken in for veterinary care and another local mountaineer, Fatima del Ãngel Palacios, is caring for Canelo until he is ready for adoption.
In the U.S., while search and rescue teams occasionally respond to pet emergencies, only a small number of organizations train dedicated animal rescue teams. The Oregon Humane Society Technical Animal Rescue Team is one such group trained to scoop pets from cliffs and extricate canine friends from forests.
It seems natural to return the favor in search and rescue. For decades, dogs have proven essential in SAR teams, from massive disaster searches after earthquakes to tracking lost hikers or humans missing in avalanches. The International Search and Rescue Dog Organization represents 126 national search and rescue dog organizations from 43 countries. The U.S. has also established standards for SAR dog team training and certification with organizations such as Search and Rescue Dogs of the U.S. (SARDUS) and the Federal Emergency Management Agency (FEMA) Canine Subgroup.
Smaller branches organize teams by region. SARDUS Colorado certifies specialized dog teams including Wilderness Air Scent (trained to search 160 acres in two hours), Water Search (both shoreline and open water drownings), Avalanche, and Disaster Dog Teams. Certifications require skill assessment tests to meet the SARDUS criteria of superior standards. Avalanche certification requires a dog capable of searching for 24 hours in extreme weather and covering one acre of snow terrain in thirty minutes for multiple victims.
Dogs seem to embrace and even enjoy the challenge. Recently, Parks Canada’s rescue team German Shepherd tracked a lost hiker over 22 kilometers in the snow. While rescue team members thought further search might be impossible, canine champ Leroy had energy to spare, and was ultimately able to help find the missing person.
In the case of Mexico’s famous new mountain climber, Canelo may be the first known dog to summit Pico de Orizaba. The canine social media sensation has already received overwhelming adoption offers and will likely have no problem finding a new home.
Cave Rescues and Hypothermia: Lessons from a Rescue in Southern Wales
Brennan Enright, MS-III,
The University of Arizona College of Medicine
Written on November 19, 2021
In early November, one of the longest cave rescues in the UK occurred in the Ogof Ffynnon Ddu cave system in South Wales. Also known as Cave of the Black Spring, it is one of the deepest cave systems in the UK at 274 meters deep and well-known to experienced cavers.
The rescue involved nearly 300 volunteers from ten different rescue teams from across the UK and ultimately took 54 hours to finally get the subject to safety. The subject, a fit and experienced caver, stepped on a rock that shifted causing him to fall eight meters and suffer fractures of his tibia, fibula, and jaw, as well as non specified injuries to his chest and spine prompting the need for extrication via stretcher. Further complicating the scenario, his initial entry point to the cave was too narrow to fit a stretcher and rescue teams, so he had to be taken the long way out: over two miles of narrow passages, caverns, rappels, pools, and waterfalls.
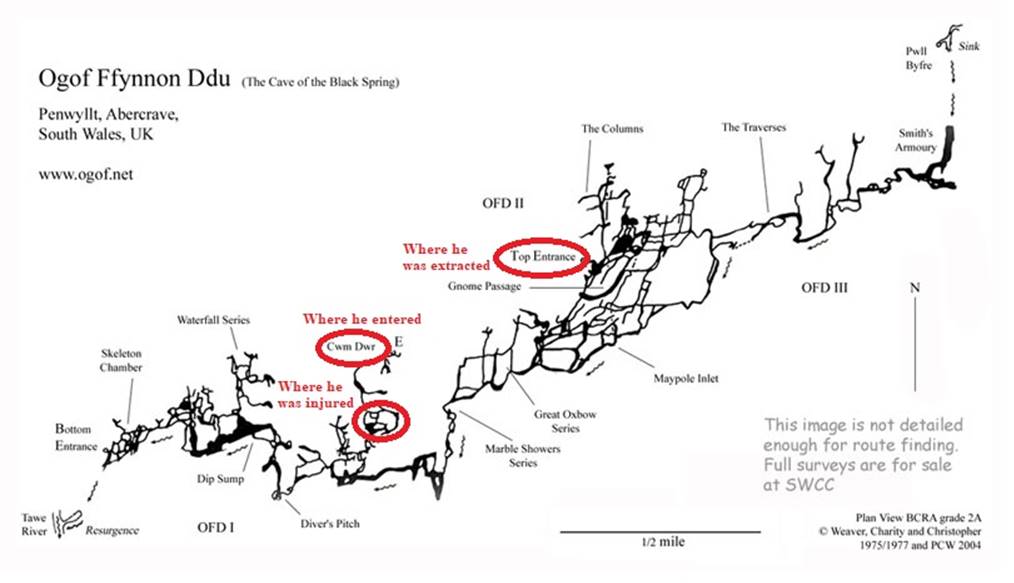
Above-ground litter rescues can be arduous and time-consuming tasks requiring significant manpower and large teams to share the work. In cave rescues such as these, the numerous constrictions, waterfalls, pools, and drop-offs require even more work with constant raising, lowering, and rearranging of the subject. The rescue team had to often use unconventional techniques such as lying down to provide a surface to slide the stretcher across or rigging rope systems to pull the subject through single-person squeezes. On top of that, the cave’s many waterfalls and pools made it prone to flooding, causing the teams to constantly re-route to mitigate risk and attempt to keep the subject and rescue teams dry.
Additionally, since radios do not work underground, the teams used Cave Link, a Through-the Earth (TTE) type of radio signaling that utilizes ultra-low-frequency waves which more readily penetrate dirt and rock. This system allowed rescuers to send text messages between the surface and within the cave in order to efficiently coordinate logistics without having to send members of the rescue team to the surface to convey messages.

Credit: South & Mid Wales Cave Rescue Team
When the medical team reached the subject, they assessed his injuries, splinted the fractures, and quickly assessed for hypothermia. When hypothermia is a concern, it is important to consider methods to mitigate the different types of heat loss that can occur - radiation, convection, conduction, evaporation and the unique contributions a cave environment makes to each:
Radiation:
The body can lose about 60-70% of its heat through radiant heat loss to the air. With the Ogof Ffynnon Ddu cave averaging 9°C, rescuers were attentive to insulate the subject, even bringing down a heated vest. This vest actually ended up being needed by one of the rescuers - further proving the risk this environment posed to rescuers as well.
Convection:
The body loses roughly 10-15% of its heat through convective heat loss. Due to the relatively constant temperature inside of caves and the fluctuating temperatures outside, a constant draft often exists in caves, making main passages rather windy. This makes it important to limit the subject’s exposure and shelter in side passages or alcoves when not moving.
Conduction:
The body generally loses around 2% of its heat through conduction with the air, but this is greatly increased when the body is conducting heat via the cold ground. The subject was initially found lying on the ground after which he was immediately transferred to an insulated pad--and ultimately an insulated stretcher - preventing conductive heat loss with the ground.
Evaporation:
Evaporative heat loss can cause up to 85% of body heat loss when a person is wet. This cave system is a humid environment with numerous pools and waterfalls-- being described as “long, cold, and wet” in an online guide. To minimize evaporative heat loss, rescuers removed wet clothing and covered the subject in a tarp to keep him dry while continuously monitoring flood risk in the main passageways. Respiration, a type of evaporative heat loss, can account for up to 30% of total heat loss. In this rescue, there are reports that an inhalation rewarming device was used to provide heated air for the subject to breathe.
Late the next evening, after over 50 hours of work, the subject was successfully extracted from the cave where he was then brought to a hospital where he is expected to make a full recovery.
Deadly Avalanche on Chimborazo, Ecuador Highest Peak
Thuy-Vi Nguyen, BA
MS-I, University of Miami Miller School of Medicine
Written on November 14, 2021
At 6:00 a.m. on the morning of October 23, 16 climbers were struck by an avalanche on the west face of Chimborazo, Ecuador’s highest peak. Climbers were ascending via the Standard Route when an avalanche was triggered at approximately 20,013 feet on the 20,548-foot mountain. On most recent reporting, Ecuador’s Integrated Security Service, ECU 911, and Quito firefighters have stated that three people have died, three are still missing, and the remainder of the party of twelve were rescued, all Ecuadorian nationals.
Search and rescue operations were coordinated by the Special Operations Group composed of staff from police and fire departments as well as the Ministry of the Environment. As of November 4th, another avalanche on the peak had delayed further rescue efforts, but a spokesperson from Aseguim, the Ecuadorian Association for Mountain Guides, reaffirms that the search will continue once conditions stabilize.
Chimborazo, located 80 miles south of the capital of Quito, typically has year-round snow coverage. Additionally, the peak’s corniced summit and steep grade can lead to dangerous conditions. Ascension up the Standard Route is no longer the safest approach as climate change has led to a rapidly shrinking glacier and a subsequent increase in rockfalls.
Chimborazo had received over two and a half feet of snow three days before the avalanche. The avalanche was believed to be triggered by weather conditions, particularly snow melt. Volcanic activity was not thought to be at play.
This avalanche represents the deadliest accident on the peak since November 1993, when ten climbers were killed at the same location. In 2015, the remains of three of those climbers were found at 16,000 feet.
Ecuador’s Ministry of Environment responded by suspending all mountaineering above 16,404 feet until November 12 or until conditions stabilize. In addition to Chimborazo, this temporary ban includes other popular mountaineering peaks such as Cayambe, Cotopaxi, Illiniza Sur, and Antisan.
Since the ascent does not require technical climbing techniques, Aseguim reaffirms that all climbers should still ascend with registered guides, consider other routes (because the Standard Route is traditionally the fastest route), and be mindful of weather conditions. Additionally, in response to the avalanche, Aseguim will begin releasing a biweekly snowpack and conditions report.
As the Northern Hemisphere begins to enter winter recreation season, review of avalanche safety is paramount.
Before going out to the backcountry, recreationists should check and learn how to read local avalanche forecasts, which are typically available through regional backcountry avalanche centers. At minimum, recreationists should be familiar with the five-level Avalanche Danger Scale that provides daily danger ratings of low, moderate, considerable, high, or extreme. Forecasts also provide information on the likelihood of avalanches, expected size, and travel advice.
Recreationists should also understand why avalanches happen and how to recognize the five signs of unstable snowpack. For an avalanche to occur, three conditions must be met: there must be unstable snow, you must be in avalanche terrain, and there must be a trigger. Avalanche forecasts can be one reliable source of information on snowpack stability. Recreationists should be familiar in recognizing avalanche terrain and should consider the steepness of the slope, whether slopes are connected, and terrain traps such as gullies, rocks, cliffs, and trees.
Terrain traps are also of particular concern since they increase the risk of injury due to collision and can make rescue more difficult. Since most avalanche deaths are due to trauma or asphyxia due to being buried, terrain traps have the potential to exacerbate these risks. Finally, triggers might be natural in origin, such as precipitation or wind, but most avalanche accidents are triggered by people moving on unstable snow.
Five warning signs of unstable snowpack include recent avalanches, shooting cracks, sound, weather changes, and persistent slab avalanches. When in doubt, it is best to assume that any avalanches were recent, which can often be identified by chunky avalanche debris or fracture lines along vertical faces where avalanches have pulled away from snowpack. Shooting cracks might run for up to hundreds of feet and are often accompanied by “whumpfing,” or the sound of unstable snowpack that is caused by air rushing out. Persistent slab avalanches, caused by a weak layer of snow buried under other layers, are particular dangerous after recent storms.
It is suggested that all recreationists carry rescue gear and supplement their knowledge with avalanche safety classes. Recreationists should carry a transceiver, which would allow them to locate members of their party, a snow probe to pinpoint someone who is buried, and a shovel. There are several organizations that offer courses that progress from avalanche awareness to more advanced field courses. Learning about avalanche safety is a lifelong process and education goes a long way in accident prevention.
Physician Charged with False Report to Facilitate Wilderness Rescue on Denali
David Gordon, W-EMT, EDAC
MS-I, Sidney Kimmel Medical College, Thomas Jefferson University
Written on November 14, 2021

(https://mountaintrip.com/wp-content/uploads/2017/05/Denali-Upper-Mountain-Route-Map.jpg)
During a May 2021 summit attempt on Denali’s popular West Buttress Route, Dr. Jason Lance, a Utah physician, had joined a new climbing partner at camp. As they ascended, his climbing partner experienced symptoms of altitude sickness and fell 1,000 feet, prompting helicopter rescue by the National Park Service. As Dr. Lance was descending back down the mountain with a separate group, Dr. Lance is alleged to have falsified a report of shock and hypothermia to facilitate self-rescue. On November 9, Dr. Lance was charged in Federal Court with falsifying the report, interfering with a government employee, and violating lawful order.
While attempting to summit, Dr. Jason Lance’s climbing partner, Adam Rawski, began to experience symptoms of altitude sickness between 18,600 and 19,200 feet. Dr. Lance joined Mr. Rawski that day as an “ad-hoc climbing team,” which form as climbers seek partners to make it to the summit, but may often lack an understanding of one another’s limitations and technical skills. When Dr. Lance encountered another two new climbers, Dr. Lance left Mr. Rawski to continue to attempt the summit on his own. At some point, Dr. Lance had taken Mr. Rawski’s Garmin inReach satellite communications device. Dr. Lance later abandoned the solo summit attempt and rejoined the group to descend Denali Pass.
On the descent, Dr. Lance and Mr. Rawski were not using a rope. Dr. Lance noticed that Mr. Rawski was no longer behind him on the descent and he saw a climber motionless at the bottom of the Autobahn glacier. Mr. Rawski had fallen 1,000 feet from the pass, sustaining serious traumatic injuries. Dr. Lance used Mr. Rawski’s inReach device to trigger an SOS. Climbers at high camp (17,200 feet) also witnessed the fall and reported it to the National Park Service. Fortunately, Denali’s high-altitude helicopter was nearby and quickly mobilized for a rescue, arriving within thirty minutes. Mr. Rawski was found unresponsive, but alive, and transported for life-saving treatment.
After Mr. Rawski was extricated, Dr. Lance again used the inReach device to message to send a message: “No injuries. Stuck without equipment after climber fall. Request assisst [sic] for evac.” The National Parks Service responded to descend if rope was available.
An hour later, Dr. Lance messaged the Parks Service: “Cant decend [sic] safely. Patients in shock. Early hypothermia. Cant you land east of pass?”
Dr. Lance’s message of a potentially fatal emergency prompted another helicopter to launch for rescue. However, the aircraft turned away when guides at a lower altitude camp reported three climbers, including Dr. Lance, were descending Denali by themselves. Court filings relate Dr. Lance’s fellow climbers had not reported suffering medical shock or hypothermia. The climbers attempted to convince Dr. Lance to descend, but Dr. Lance insisted on staying because the National Park Service was obligated to rescue them since “we’ve paid our fee.”
The following day at the 14,200 ft camp, a park ranger law enforcement officer interviewed Dr. Lance and attempted to collect Mr. Rawski’s communications device to return it to him. Dr. Lance responded “no” and reportedly tampered with the device. A search warrant revealed multiple deleted messages, including one citing “no injuries” and another citing a lack of proper equipment necessitating a rescue. Later, the ranger asked why Dr. Lance claimed to need an airlift rescue, informing Dr. Lance that the other climbers did not report any hypothermia. As a licensed and trained physician, he responded that he could better identify early hypothermia and shock than the climbers. Still, Dr. Lance did not identify any potential treatments he provided.
Psychological readiness, technical skills, and contingency plans are necessary to summit a mountain safely. In a blog post published days after this incident, the National Park Service reiterated they will only respond to “immediate threats to life, limb, or eyesight.” For other incidents, the National Park Service “will leave you to figure it out on your own,” turning down rescue requests that do not meet immediate threat criteria. Initiating wilderness rescue is risky, especially a mountain helicopter rescue. Often, the weather may preclude a helicopter rescue until conditions are safer and operations can be hazardous for the rescuers. Although a scenario where a climbing partner falls and sustains severe injuries is likely physiologically and psychologically draining, adventurers remaining on the mountain need a clear plan to maintain a level head and descend without the expectation of rescue assistance.
**Update**
June 29, 2022
On April 1, 2022, the U.S. Attorney's Office for the District of Alaska released that Dr. Lance had pled guilty of violating a lawful order during the accident investigation of the defendant's climbing partner who fell more than 1,000 feet from the top of Denali Pass. Mountain Ranger and Law Enforcement Officer's testimony described Dr. Lance's climbing partner's rescue as one of Denali's most significant rescues in the park's history. Dr. Lance was charged with interfering the rescue operation, failing to turn over his partner's inReach communicator device, and making a false report by deleting messages requesting rescue from the inReach device. Any rescue on Denali carries inherent risks. While the rescue team was able to save the life of Dr. Lance's climbing partner, Dr. Lance's additional request for helicopter rescue was unsubstantiated.
Ultramarathoners Rescued from Unanticipated Whiteout in Davis County Utah
Corey Hazekamp, MD, EM PGY-1 Lincoln Medical and Mental Health Center
Written on October 14, 2021
The Wasatch Mountain Range, just north of Salt Lake City in Davis County, Utah is home to Davis County’s 50-Mile Ultra Marathon or the “DC Peaks 50.” The DC Peaks 50 was created to be a grueling trail running race which starts at East Mountain Wilderness Park in Kaysville, Utah and requires runners to conquer 11,700 feet of elevation gain and 8,367 feet of descent and finishes in Tunnel Springs Park, Utah. The race was designed by ultrarunners and advertises strenuous geography that requires grit and persistence to complete the course which comprises mostly rural trails with only 24% of the race being on service road and 2.5 of the 50 miles on paved roads. The race includes running over the summits of Francis Peak (9,560 ft) and Bountiful Peak (9,143 ft), both in the Wasatch Range.
As October 9th, the race day, approached, 87 participants planning on running the inaugural race were instructed to prepare for some rain and a possible ‘dusting of snow.’ Several hours into the race, heavy snow began to fall with winds gusting approximately 30 to 40 miles per hour. About 18 miles from the start line, it was reported that 12-18 inches of snow had fallen and racers were faced with whiteout conditions, at which time officials suspended the race at the top of Farmington Canyon. The race was called off at 8:30 AM and the first racer call for help arrived around 9:30 AM, approximately 4.5 hours after the 5 AM start time of the race. Rescuers were dispatched to scour the entire racecourse on foot, in four-wheel-drive vehicles, and on snowmobiles to find all 87 participants. By 2:45 PM, all the runners were accounted for. One participant suffered a minor injury from a fall, a few racers were treated at the base of the mountains for hypothermia, and all 87 racers were released from the scene without hospitalization. Jordan Stuart, a participant in the DC Peaks 50 race, posted a video showing the conditions experienced during the event.
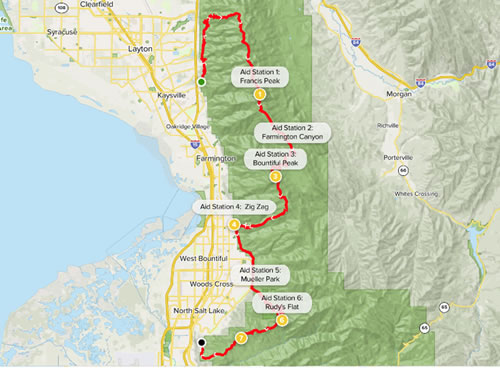
This occurred less than five months after the tragedy at the Yellow River Stone Forest Park in Gansu Province of China where 21 of China’s top marathon athletes died, succumbing to freezing rain and high winds. Luckily, there were no fatalities during the unexpected conditions experienced during the DC Peaks 50. Temperatures dropped to about 20°F (-7°C) and some participants reported feeling more miserable about weathering the conditions knowing they’d be helped rather than fearing for their lives. The last member of the rescue team exited the racecourse at 7 PM due to difficulty navigating treacherous conditions coming off the mountain.
Care Consideration for Ultramarathon Runners
The WMS Breaking News section recently highlighted how ultramarathoners are at an increased for hypothermia. With the forecast in Davis County originally calling for mostly rain during the DC Peaks 50 and the participants running at higher altitudes, they were vulnerable to suffer from a wide range of wet and cold-related illnesses. In addition to hypothermia, medical staff was likely on the lookout for frostbite, chilblains, and trench foot.
Chilblains are superficial injuries that affect bare skin which is exposed to the cold, presenting as painful or itchy erythematous papules most commonly on fingers, ears, and shins and is associated with a prolonged burning sensation. If the racers had been exposed to rain, some of the 87 runners would have most likely experienced trench foot. Trench foot should be considered when runners are exposed to wet and cold temperatures (0-15°C or 32-59°F) for prolonged times (12 hours to 4 days). Early symptoms include red and swollen feet with or without numbness. As severity increases, trench foot will progress to pale and cyanotic appearing feet. Treatment of trench foot includes removing wet socks and shoes and exposing the feet to dry air. Runners should be educated that changing their socks and/or shoes 2-3 times during an ultramarathon can help prevent trench foot.
Manual Inguinal Compression to Reduce Hemorrhage After Shark Bite
Austin Martin, MS, AWLS, OMS-II
Written on Oct 11, 2021
An Australian EM physician has discovered a simple yet highly effective method to limit hemorrhage after a shark bite to the lower extremity. Dr. Nicholas Taylor, Associate Dean of the ANU Medical School and himself a surfer, was the first author on the study. Inspired by a series of shark attacks on surfers in Western Australia during a family vacation, Taylor utilized his emergency medicine training to devise a novel method to assist surfers in the event of a lower extremity shark bite. The technique requires a single rescuer and no additional equipment; it is meant to limit the patient's blood volume loss prior to the arrival of additional rescuers and transport to definitive medical care.
Shark bites can cause complex neurovascular and muscular injuries. Many of the current guidelines to acutely treat lower extremity hemorrhage due to shark bites involve applying manual pressure directly to the wound. The effectiveness of this method greatly depends on the particular injury; every shark bite injury is unique. Sharks have multiple rows of teeth and therefore can produce innumerable puncture wounds and lacerations to underlying vascular structures. These complex injuries can become an issue if the rescuer attempts to tamponade the wound directly since it may be impossible to occlude all portions of damaged vessel(s). The method that Dr. Taylor and his team published involves reducing blood flow through the femoral artery directly rather than applying pressure to the more inferior wound (see below figure). The technique requires constant body-weight pressure of the rescuer’s fist on the patient’s mid-inguinal point to occlude the femoral artery.
"I knew from my background in emergency medicine [that] if people have massive bleeding from their leg, you can push very hard on the femoral artery and you can pretty much cut the entire blood flow of the leg that way.
"If someone has been bitten on their leg, you only need to find the middle point between the hip and the genitals, make a fist and push as hard as you can.
"We found people can do this for a long period of time and making a fist covers the area you need. It's not hard to find,” Dr. Taylor says.
The study, published in Emergency Medicine Australia, compared reduction of femoral blood flow from surfboard leg leash tourniquets to that of inguinal external compression in 34 volunteer subjects. Doppler ultrasound was utilized to record the reduction in popliteal artery peak systolic velocity. Dr. Taylor et al. found that inguinal compression was superior to leg leash tourniquets and resulted in a significant reduction in popliteal artery peak systolic velocity (P0.001). In fact, 75% of their measurements achieved 100% reduction of flow. On average, the technique achieved 89.7% reduction in blood flow compared to only 43.8% reduction by leg rope tourniquet.
"Most people could completely stop all blood flow. This new method saves time and works better than using a leg rope or looking for something else to use as a tourniquet," Dr.Taylor said.
The study also compared the effectiveness of the technique with and without wetsuits; ultimately there was no significant difference.
"I want posters at beaches. I want to get it out in the surf community. I want people to know that if someone gets bitten you can pull out the patient, push as hard as you can in this midpoint spot and it can stop almost all of the blood flow."
Limiting hemorrhage quickly can be a critical factor in the survival of a patient who suffers from serious shark bites. Although some limitations exist, such as difficulty to perform during transport and provider fatigue, this novel technique may lead to increased survival of surfers and others who recreate in waters where sharks are native.
A Vaccine for Lyme Disease is on the Horizon
Kylie Van Hoesen, MS-IV, University of Colorado Anschutz School of Medicine
Written on October 9, 2021
Lyme disease is transmitted to humans through the bite of the Ixodes tick, which are predominately located in the Northeastern region of the U.S. Estimates suggest that 476,000 people are treated for Lyme disease in the U.S. each year. Common manifestations of Lyme disease include the classic target-like rash (erythema migrans) along with non-specific symptoms of fatigue, fever, headache, and joint pain. However, some patients can present with more severe symptoms including carditis and neurologic disease. An estimated 10-20% of patients have symptoms that persist months to years after treatment with antibiotics.
The effects of climate change and increased land development have increased the geographic range of ticks carrying Lyme disease which is contributing to the increased burden of Lyme disease in the U.S. Additionally, the economic impact of Lyme disease is an important consideration as it costs the U.S. healthcare system nearly $1 billion every year, averaging $3000 per patient.
Currently, preventing Lyme disease and other tickborne diseases comes down to preventing tick bites. In Europe and Asia, there are a few vaccines against tickborne illnesses, however, none are currently available in the United States. There was a previous vaccine against Lyme disease, known as LYMErix, that was developed in 1998 and targeted a specific protein on the bacteria (known as OspA). It was removed from the market by the manufacturer in the early 2000s due to decreasing public demand in the midst of side effect concerns and emerging vaccine hesitancy. Early initial individual case reports indicated that LYMErix may have had side effects including polyarthritis, although larger studies did not support these claims. Now with funding from the NIH of more than $6 million for tick prevention projects, there are two emerging options:
- A new Lyme disease vaccine similar to LYMErix: Pfizer is co-developing a vaccine with Valneva that targets six serotypes of Lyme, covering strains both in the U.S. and Europe, now in Phase II clinical trials. The goal will be vaccine availability in 2025.
- Pre-exposure prophylaxis (PrEP) through human monoclonal antibodies: MassBiologics is developing Lyme PrEP that has undergone Phase I clinical trials. Monoclonal antibody vaccines are beneficial as they essentially skip the step of inducing the body’s immune system to produce antibodies and instead provide the antibodies within the injection to kill the Lyme bacteria (Borrelia burgdorferi). The vaccine will most likely require a yearly booster. Further clinical trials will elucidate effectiveness and possible side effects, though monoclonal antibodies typically carry lower risk for side effects. The projected timeline is for availability in 2024.
- Tick-focused approach: There has been some ongoing research and discussion of vaccine strategies targeting the tick itself which would allow prevention of several tick-borne diseases and reduce co-infections. The approach would be to target tick salivary proteins to block their feeding, effectively reducing transmission of the pathogen from entering the human host.
One major question that remains is if people get the vaccine? With current conversations around the COVID vaccines, it will be interesting to see how future vaccines are adopted by the public. Unlike COVID, Lyme is a non-communicable disease making the Lyme vaccination a more personal decision for those living and recreating in endemic areas. Although there are effective tick prevention strategies and treatment options for Lyme disease, the options remain limited. The incidence of the disease will continue to increase substantially and vaccination efforts will likely be an important method of preventing both Lyme and other tickborne diseases moving forward.
Emergency Physician Performs Field Tracheotomy on Mountain Biker
Dominique Gelmann, BS
Written on October 4, 2021
On September 12, 2021, Dr. Jesse Coenen hit the Cuyuna Lakes Mountain Bike Trails in Minnesota, intending to cycle off the demands of his recent 13-hour shift as an emergency physician.
Todd Van Guil another local mountain bikerhad similar plans to enjoy an autumn ride in the same park with his friend. Neither rider anticipated the events that actually transpired in the woods that day.
According to news reports, Van Guilder unfortunatelysustained a crash, striking his chest and abdomen on the ground after launching from his bicycle. As he sat up, he noticed difficulty breathing and spotty vision that prevented him from seeing his friend. His companion quickly called 911 as the severity of the crash became evident. Six paramedics arrived on scene soon after and sent an accompanying police officer back to the parking lot for an oxygen tank after assessing Van Guilder’s respiratory status.
Dr. Coenen, who happened to be riding down the same trail, crossed paths with the police officer at just the right time. After hearing about the urgent situation, he biked to the crash site and performed a rapid assessment of the now unconscious Van Guilder and the surrounding scene. Coenen quickly determined the need to secure an airway and stepped in to assist the paramedics. After several failed intubation attempts due to poor visualization, he made the critical decision to perform a field tracheotomy. Though he had never performed one on a real patient, he successfully executed the procedure and Van Guilder’s oxygenation status improved.
The injured biker was safely transferred to a hospital by helicopter, where he was treated for TBI and discharged 10 days later in good condition.
A testament to teamwork and Dr. Coenen’s ability to practice in austere conditions, the wilderness resuscitation succeeded in saving Van Guilder’s life.
“I’m obviously extremely fortunate that [Dr. Coenen] happened to be there that day at that precise moment,” he reported to the media. Without the collaborative effort and the physician’s skills on the trail, Van Guilder’s bike ride may have resulted in a much less favorable outcome. “It’s a lesson to us all that you never know who you’re going to encounter,” said Coenen.
Wilderness Airway Management
As is true in most airway emergencies, simple positioning maneuvers such as the rescue position and jaw thrust and chin lift may first be attempted with or without the use of bag-valve mask device.
In spontaneously breathing patients, an oropharyngeal or nasopharyngeal airway may augment ventilation.
Endotracheal intubation is attempted when spontaneous respirations are not present or the airway is not protected. Blind nasal intubation could be considered without a laryngoscope although can be difficult to achieve.
The Difficult Airway Society guidelines indicate that when tracheal intubation cannot be accomplished, placement of a supraglottic device, such as an LMA, could be attempted next. If this method fails to provide adequate oxygenation, a surgical airway may be considered. In certain emergency circumstances, a surgical method is indicated as the initial step in airway management.
Emergency Tracheotomy
A tracheotomy is the surgical creation of an opening into the trachea, which may be required if other options fail or when a surgical airway is inevitable. The procedure is performed by making a 3-4 cm vertical midline incision below the cricoid cartilage to expose the trachea, through which an airway can then be inserted.
A tracheotomy allows for establishment of an airway placed below the glottis, typically between the second and third tracheal rings. Image source: New England Journal of Medicine.

(click to watch video)
Percutaneous Tracheotomy performed in the hospital setting. Video source: New England Journal of Medicine.
Field Considerations
Austere conditions present unique challenges to an already demanding emergency procedure. Typical options for anesthesia may not be available, for example. In these cases, local anesthetic may be sufficient in an unconscious patients and verbal reassurance may allow for its sole use in awake individuals as well.
An awake procedure can be performed with or without ketamine depending on availability and clinical setting.
Standard equipment may not be available and creativity is often necessary. In a
particularly remarkable example, a pair of physicians successfully intubated an injured hiker in the wilderness using tubing from a hydration pack. Despite prior speculation that ballpoint pens may be effective alternatives to tracheotomy tubes, the internal diameter of most common pens provides
too much airway resistance to provide adequate airflow. Even for appropriately sized pens, the cricothyroid ligament is
nearly impossible to penetrate with this method. While attaining an ideal sterile field is impossible in the wilderness, skin decontamination should be performed using appropriate available agents. Finally, consideration of patient transfer is key and the airway must be properly secured to ensure its maintenance en route to a hospital facility.
Although the exact details of the emergency field airway procedure that Dr. Coenen performed are still forthcoming and have been initially reported as a tracheotomy, it is most likely that a field cricothyroidotomy is performed in these situations.
Climbers Caught in Deadly Storm on Mt. Elbrus, Russia
Corey Hazekamp MD, EM PGY-1; Lincoln Medical and Mental Health Center
Written on October 3, 2021
An unexpected storm caught a group of climbers attempting to summit Mt. Elbrus in the Caucasus Mountains on September 24, claiming the lives of five team members. Mt. Elbrus towers 18,510ft (5,642 meters) above sea level and is notorious for unpredictable weather, claiming the lives of several climbers each year. Russia’s Emergency Ministry deployed a team of an estimated 69 rescuers on a mission to save primarily ‘non-professional’ climbers and their guides. Of the 14 members who made it off of the mountain 11 were hospitalized with two admitted to intensive care.
One member of the team was unable to summit as she turned around early with her guide due to feeling ill. Anna Makarova, 36, and in seemingly ‘perfect physical shape’ felt ill about 300m from the summit just when the weather started to take a turn for the worst as wind speeds rose and air pressure decreased. Anna was given tea and ammonia but reportedly died in her guides’ arms about 40 to 60 minutes after turning around. The remaining team members made it to the summit only to be caught by the storm during their descent. As the team was hiking down one member broke his leg leading the guides to decide to split the team into ‘fast’ and ‘slow’ groups. According to press reports, two members froze to death and two others lost consciousness and died on their way down. The Emergency Ministry reported subzero temperatures with strong winds and poor visibility.
The Caucasus Mountains is part of the Caucasus region which serves as a natural border between Eastern Europe and Western Asia, spanning from the Black Sea to the Caspian Sea. Mt. Elbrus is the 10th most prominent peak on the planet, beating out Mont Blanc by over 800 meters to take the crown of tallest mountain in Europe. Mt. Elbrus is used as a climbing and hiking destination in the summer and serves as a ski resort in the Winter.
Though not considered a technical climb, fatal accidents occur on the mountain during summit attempts every year.
Mt. Elbrus, like much of America’s popular outdoor recreational areas, has recently experienced an influx of tourists. Per local authorities, the region experienced a 30 percent increase in visitors just in the first half of this year when compared to the first half of 2019 (pre-pandemic). As many people in our country and across the world have been more isolated during the past 18 months or working from home full-time, it's no surprise that people are craving outdoor recreation and adventures. With increasing crowds of novices adventuring to more remote areas, wilderness medicine educators will need to reinforce the importance of packing and planning for unforeseen circumstances and having emergency plans in place.
Cause of Death for California Family Found in the Sierra National Forest
April B. White, MBS, NRP, FP-C
MS-3 Geisinger Commonwealth School of Medicine
Written on September 30, 2021
A family hiking in the Sierra National Forest was found deceased amid puzzling circumstances along the Hite’s Cove Trail on August 17th. Without evidence to suggest foul play, investigations turned towards an environmental influence as a possible cause of death for the young couple, their 1-year-old daughter, and the family dog. Water samples drawn from the Merced River, which runs along the Hite’s Cove Trail, recently revealed elevated levels of Anatoxin A related to a Harmful Algal Bloom (HAB). At the time of this writing, it has not been officially announced as to whether there is a confirmed connection to the tragic occurrence.
Harmful Algal Bloom events (HAB), commonly referred to as “toxic algae,” are an invasive overgrowth of cyanobacteria species that often produce large quantities of cyanotoxins, such as microcystin and anatoxin. These events often have devastating consequences for aquatic ecosystems, wreaking havoc on native plant photosynthetic functions and oxygen levels of the water column, resulting in high mortality rates for fish and aquatic plant species. Frequently, affected water sources demonstrate a characteristic blue-green floating scum, however there are many species of cyanobacteria that form submerged mats well below the water’s surface that can be equally as disruptive and dangerous, yet not as readily visible.
Certain field water decontamination techniques may also prove ineffective against these bacterial toxins, posing risk to outdoor enthusiasts. Despite their convenience and portability, methods such as halogenation (chlorination/iodination) and filtration tend to confer greater risk of incomplete decontamination and intoxication compared to other methods such as boiling and ultraviolet (UV) oxidation (See Table 1).
Anatoxin A (ATX) is a potent cyanotoxin with toxidrome presenting similar to a cholinergic crisis. Animal studies have demonstrated that ATX has significantly greater affinity for the nicotinic acetylcholine receptor than does acetylcholine, resulting in irreversible receptor agonism. Signs and symptoms can present in as little as minutes or up to days following exposure and may manifest as peripheral numbness, tingling, burning pain, drowsiness, excessive salivation, vomiting, diarrhea, muscle fasciculations, seizures, and respiratory paralysis eventually leading to death. The majority of ATX intoxications have been studied in dogs, cattle, and waterfowl, who ingest large quantities of algae and toxin by swimming in contaminated waters and then licking themselves clean. Routes of exposure include oral ingestion of contaminated water sources, dermal absorption, and inhalation of aerosolized toxin, with oral ingestion accounting for the greatest quantity of toxin intake. Currently, there is no accepted consensus as to whether ATX can volatilize out of solution; however, a recent study in April 2021 demonstrated detection of airborne ATX during a HAB event.
Assessment and treatment for patients affected with possible ATX poisoning should encompass a thorough history with a high index of suspicion for this uncommon malady. Providers assessing patients in the field should observe strong personal safety and consider HAZMAT resources and decontamination techniques. Patients with surface exposure should be thoroughly flushed with fresh, clean water. Patient care is mainly supportive, although the use of atropine & pralidoxime to counter a cholinergic crisis may also be considered.
There are still many questions left unanswered as to what led to the tragic fate of this California family. Even as investigations are still underway, there is much we can learn as a wilderness medical community about these situations and our role in identifying, treating, and preventing further tragedies.
Take Home Points:
1. Not all Harmful Algal Blooms (HAB) are visible on the surface- look for indicators of toxin presence such as high fish and plant mortality in the area.
2. Keep a high index of suspicion when assessing patient history, especially if pets are affected as well.
3. Some field water decontamination techniques, such as halogenation and filtration, may not be sufficient against certain cyanotoxins.
4. Treatment for Anatoxin A poisoning is supportive. Consider HAZMAT resources and personal safety in field patient care. Atropine & pralidoxime may counteract symptoms of cholinergic-excess.
Table 1: General effectiveness of cyanotoxin oxidation with common water treatment oxidants.
(Source: EPA.gov)
10/22 UPDATE
An official determination in the cause of death of the California family found deceased while hiking in the Sierra National Forest in August has been released. Authorities have determined the official cause of death to be related to heat and dehydration for the young couple, their 1 year-old daughter, and family dog. Despite treating the scene as a suspected hazmat site, with potential contamination from nearby mining gas or, as previously discussed, a toxic algae bloom, these suspicions and many others were reportedly ruled out.
Reports state that the family was found all within close proximity, with an empty 84oz water container, and only a mile from the trailhead where their car was parked. Officials report that the family embarked on the six mile hike when temperatures were around 70 degrees fahrenheit, however temperatures along that trail were recorded nearing 109 degrees later that day.
Even young, fit individuals are not immune to the dangers of heat and dehydration. Possibly caught off guard with the rising temperatures over the duration of the hike, this family may have been underprepared with the amount of water that they had packed.
It is unknown if there will continue to be more developments in this story, however there is likely much more that we can learn from the tragedy that struck this family.
April 2022 Update: The initial submission included an erroneous statement that boiling could be an effective method of removing cyanotoxins. It has been removed for accuracy.
Cliff Falls in Grand Canyon Prove Dangerous and Fatal
By Pharibe Pope
Written on September 28, 2021
On Saturday, August 28, Oregon hiker David Colburn fell 50 feet to his death in Grand Canyon National Park. The incident marks the 18th fatality in the Grand Canyon this year.
Colburn fell while hiking a narrow slot canyon at Deer Creek as part of a non-commercial river trip. Hikers and river rafters have noted a difficult traverse in a narrow canyon around Deer Creek Falls, nearly 136 miles downriver from Lees Ferry, where rafting trips typically begin.
Upon receiving report of the incident, the Grand Canyon Regional Communications Center dispatched multiple teams of technical and swiftwater rescuers. Darkness and difficult terrain resulted in the teams’ need to suspend the search overnight. The following day, Colburn’s body was found and transported via helicopter to the South Rim. The National Park Service and the Coconino County Medical Examiner’s Office continue to investigate the incident.
An average of 12 deaths occur each year in the Grand Canyon stemming from medical conditions, heat exhaustion, drowning, and other dangerous environmental conditions. Typically two to three of those causalities are the result of cliff falls, often from the rim of the canyon, where visitors risk uneasy footing for photo opportunities.
In response to prior cliff fall fatalities in Grand Canyon National Park, the National Park Service has encouraged visitors to stay on “designated trails and walkways, always keeping a safe distance from the edge of the rim, and staying behind railings and fences at overlooks.”
Not all falls in the Grand Canyon have resulted in fatalities, though. In 2009, a 38-year-old woman fell 50 feet from the South Rim and survived without life-threatening injuries.
There is limited reported data on wilderness falls (compared to urban falls) and information as to why the outcomes of wilderness falls vary and how medical professionals might respond accordingly. As the sport of rock climbing and visits to national parks grow increasingly popular, wilderness falls prove more common and more fatal reason this information is necessary now more than ever.
While the data is sparse, experienced search-and-rescue ranger Bil Vandergraff, a former Grand Canyon National Park ranger of 25 years, has offered helpful advice to minimize the risk of cliff falls: “Mind your feet” is rule number one. Picking up feet instead of dragging them, even when exhaustion kicks in, is critical to maintain balance. Similarly, “fit joints are healthy joints.” Improving balance and working out while training for the trail tremendously reduces the risk of wilderness falls in general. Wearing boots or trail runners with good traction is also a must. Deeper lugs work best on soft ground whereas rubber soles hold up on rocky terrain and slickrock. And lastly, move slowly. Taking time to pick a path clear of drop-offs and to navigate loose footing can mean the difference between a fun day and a fatal fall.
Media:

South Rim of Grand Canyon National Park (https://www.nps.gov/grca/planyourvisit/directions_s_rim.htm)

Deer Creek Narrows, Grand Canyon National Park
(https://www.nps.gov/grca/learn/news/visitor-fatality-at-deer-creek-august-2021.htm)
Melioidosis Cases in the U.S.
Brad L. Bennett, PhD, WEMT, Paramedic, MFAWM
Written on August 11, 2021
The Centers for Disease Control and Prevention (CDC) just released a media statement on August 9, 2021 confirming a new fatal case of the rare disease melioidosis caused by Burkholderia pseudomallei, a bacteria found in moist soil and water.
This most recent case in Georgia follows other recent cases in Kanas, Texas and Minnesota. B. pseudomallei is not considered transmissible by air or respiratory droplets. Person-to-person transmission risk is considered extremely low.
It is believed that contact through damaged skin with polluted soil or water is the most frequent route for natural infection. Healthcare personnel are generally not at risk if they follow standard precautions.
Two of the four patients, including children, had no known risk factors for melioidosis and two died. It appears all cases are linked based on genome sequencing of the bacterial strains. These strains found in the US appear related to strains found in southern Asia. None of these patients had recently traveled internationally. The CDC suspects the likely cause is an imported product (such as a food, drink, medicine, or personal care or cleaning product) or an ingredient in one of those products.
Melioidosis symptoms are nonspecific and vary depending on the type and site of infection. Symptoms may include localized pain or swelling, fever, ulceration, abscess, cough, chest pain, high fever, headache, anorexia, respiratory distress, abdominal discomfort, joint pain, disorientation, weight loss, stomach or chest pain, muscle or joint pain, and seizures. Initial presentation of the four melioidosis cases in the US ranged from cough and shortness of breath to weakness, fatigue, nausea, vomiting, intermittent fever, and rash on the trunk, abdomen, and face. Mortality varies depending on disease severity and clinical presentation, with case fatality ranging between 10-50% worldwide.
The following underlying medical conditions may increase the risk of Melioidosis: diabetes, liver or kidney disease, chronic lung disease, cancer or other condition that weakens the immune system. The CDC states that people experiencing cough, chest pain, high fever, headache or unexplained weight loss should see their doctor. The CDC is asking clinicians to watch for any acute bacterial infection that doesn’t respond to normal antibiotics and consider melioidosis regardless if the patient traveled outside the United States. The CDC also urges clinicians not to rule out melioidosis as a possible diagnosis in children and those who were previously healthy and without known risk factors for melioidosis.
CDC Recommendations:
- Consider melioidosis diagnosis in patients with a compatible illness, even if they do not have a travel history to a disease-endemic country.
-
Culture of B. pseudomallei from any clinical specimen is considered diagnostic for melioidosis. Ideal specimens for culture include blood, urine, throat swab, and, when relevant, respiratory specimens, abscesses, or wound swabs.
-
When ordering specimen cultures to diagnose melioidosis, advise the laboratory that cultures may grow B. pseudomallei and that appropriate laboratory safety precautions should be observed by the laboratory personnel.
-
Laboratory testing involving automated identification algorithms (e.g., MALDI-TOF, 16s, VITEK-2) may misidentify B. pseudomallei as another bacterium. The isolate from the Texas case was initially misidentified as B. thailandensis by MALDI-TOF. Consider re-evaluating patients with isolates identified on automated systems as Burkholderia species (specifically B. cepacia and B. thailandensis), Chromobacterium violaceum, Ochrobactrum anthropi; and, possibly, Pseudomonas species., Acinetobacter species, and Aeromonas species.
-
Treat melioidosis with IV antibiotics (e.g., ceftazidime or meropenem) for at least two weeks. Depending on the response to therapy, IV treatment may be extended for up to eight weeks. Intravenous treatment is followed by oral trimethoprim-sulfamethoxazole (TMP/SMX) for three to six months to prevent relapse. Amoxicillin/clavulanic acid can be used in persons with a contraindication to, or who cannot tolerate, TMP/SMX.
-
If B. pseudomallei is identified or an organism is suspicious for B. pseudomallei, contact your state or local public health department immediately. The health department can facilitate forwarding the isolate for confirmation to the closest reference laboratory and initiate a public health investigation.
For more information on melioidosis, visit cdc.gov/melioidosis/index.html.
Western Europe and Central China Flooding: A closer look at the health toll of climate change
Alexandra Herndon, MD
Written on July 23, 2021

Rhineland-Palatinate, Germany
Source: CNN
Recent severe rainfall has caused devastating flooding in western Europe and central China. Floods in Germany and the Benelux countries have seen losses of at least 120 lives, with 1300 people still missing. Updates from China are still developing but initial reports show entire neighborhoods have been submerged and over $190 million in economic damage has been done. These serve as grave reminders of climate change and the toll it has on our health on this planet. Flash floods, landslides, and associated damage to local infrastructure all play their parts in leaving many residents unable to escape the rising waters, as well as thousands more without power, transport, and basic means to care for themselves. Furthermore, a recent study in Nature Climate Change by NASA and the University of Hawaii has shown that changes in the moon’s orbit may also lead to more record flooding in the next decade, leaving us unable to escape the health effects incurred from these inevitable natural disasters.
When it comes to flooding, the toll of short-term and long-term health effects is wide ranging. After Hurricane Maria hit Puerto Rico in 2017, the initial death toll was reported at 64, however when taking into account not just the immediate impact but also the indirectly-related downstream effects in the ensuing months, that number tabulated to nearly 3300 deaths. While floods are not hurricanes, they are the most common natural disaster across the world and are expected to worsen as sea levels rise and extreme weather increases.

Chongqing, China
Source: France-Presse - Getty Images
Wilderness medicine has significant overlap with disaster response medicine given its expertise in providing care in limited access and under-resourced locations, often encountered in floods. Knowing the health impacts from these events allows the initial response to be tailored appropriately. In the short-term, the most common morbidity and mortality observed in floods is from drownings, hypothermia, traumatic injuries, and wounds incurred from initial flood damage. Providers giving initial support for flood victims should plan on having the proper resources for these issues such as equipment for field re-warning of hypothermic patients, initial resuscitation of drowning victims, as well as wound treatment and prolonged care if hospitals are at capacity or difficult to access.
Beyond the most immediate injuries from disasters of this scale, there are further long-term health effects. Often, there is a significant loss of healthcare workers, evacuation and transport resources, and of overall health infrastructure needed to provide necessary care. In time, wounds can become infected, communicable diseases spread due to breakdowns in sanitation and tainted water supplies, and starvation ensues due to loss of access. As communities try to repair themselves structurally, management of chronic disease falls to the wayside and at-risk populations are displaced and fall susceptible to mental health disparities and poverty as a result from the trauma and loss imposed by disaster.
The importance of recognizing not only how we can help in the immediate aftermath of these climate-related disasters but also what we can do now to prevent further health detriment due to climate change is vital. While the initial destruction laid out can be striking, the devastating long-term health effects can be even more costly than what is initially most apparent.
Falling trees claim lives of tent and hammock campers.
By Janet Peterson, DrPH, RDN, WEMT, FACSM
Written on July 12, 2021
In the last few months, there have been several instances of people being killed by dead trees or branches while camping. Recently, a 20-year-old died when a tree fell on his primitive camp spot in Florida. Two women camping in Idaho were seeking refuge in their car when a storm rolled through and a tree limb fell on the car- killing one and seriously injuring the other. In New Hampshire, a tree fell on a man while he was sleeping in his hammock.
Growing up, my father taught me to assess the viability of the trees near a spot I wanted to camp. He told me to be aware of the "widowmakers". For him, this meant not putting up a tent near an unstable tree that was either dead or dying. Defined as a detached or broken limb or tree top, the term "widowmaker" or "fool killer" comes from the forestry industry. In the wilderness environment we generally extend that definition to any dead or dying tree.
Avoiding falling limbs while camping
When setting up a tent or choosing a camp spot, evaluate the trees around you to minimize the chances of a widowmaker falling on the tent.
Check the weather before you go. If storms with high winds are predicted, think about postponing your trip or choosing a location with a lower risk of falling trees.
Hammocks are not new; historians trace the use of hammocks for sleeping to 406 B.C. Hammock camping has increased in popularity in the past few years. Hammocks are ecologically friendly by allowing you to set up camp away from high impact areas.
Choosing the right tree to suspend your hammock is important for your safety and for the health of the tree.
- Choose trees that are healthy and alive. Avoid trees with signs of damage, rot, or loose branches. Also evaluate the trees surrounding your hammock spot.
- Choose a tree that is mature enough to support the hammock. Some suggest using diameter as a guide: a minimum of 6" is recommended by some manufacturers. One camping enthusiast suggests if you can shake the tree, it is not mature enough to hang the hammock.
- Avoid poisonous plants and look for insect nests.
- Look for hazards on the ground that you will need to avoid when getting in and out of your hammock.
- Avoid hanging your hammock across animal (or human) trails.
- Use wide suspension straps to avoid damaging the outer bark essential to the tree’s health.
- Connect only one hammock to a tree. Avoid multiple hammocks attached to one tree as this increases the stress on the tree (see photo below). The fun hammock ladders (multiple hammocks stacked on top of each other) may look cool but they also increase the risk of injury both from failing trees and from mishaps when trying to get in and out of the hammock.
- Be careful selecting trees for setting up a hammock at night. It might be best to skip setting up the hammock and sleep on the ground until you can safely assess the trees.

Heat Dome in the Pacific Northwest: Record-setting heat brings clinical and informational risks.
Timothy Durkin, DO, FAAEM, CAQSM
Written on July 2nd, 2021
With record-breaking high temperatures, heat domes, and heat waves around the country this summer, outdoor enthusiasts should be watching out for two heat-related threats: heat stroke and bad information on heat stroke. Currently, a "heat dome" is sitting over the American pacific northwest and southwestern Canada: the region is experiencing record highs and temperatures that are 40ºF (22ºC) higher than average. A heat dome is a mass of hot air that becomes trapped in an area under a high-pressure system. It is caused by strong temperature gradients coming off the Pacific Ocean.
A recent high temp of 116ºF at the Portland airport on July 1st crushed the prior day’s record of 112ºF; prior to this year the highest recorded temperature at PDX had been 107ºF in August 1981. This heat wave has already resulted in hundreds of deaths: at least 79 heat-related fatalities have already been reported in Multnomah County, OR, and more than 300 sudden deaths over typical averages during a 5-day period in British Columbia, Canada. This is causing an unprecedented strain on hospital and healthcare systems in an area not accustomed to dealing with heat-related illnesses. Additionally, the heat has compromised other infrastructure including roads, bridges, public transportation and the power grid. It has also sparked several wildfires in an area already plagued with drought.
Understanding Heat Stroke
Heat stroke is an immediately life-threatening condition where the body’s temperature regulation system fails and core temperature climbs to higher than 40ºC. At these temperatures, people have very limited time to act before irreparable damage occurs to the brain, liver, and other essential organs - the body’s proteins are being “cooked” and denatured in the high core temperatures. The best treatment is immediate and aggressive cooling by immersion in ice water or the most aggressive means available. Delays in cooling, such as for hospital transport, are associated with high mortality and longer ICU stays, while rapid cooling on scene is associated with near 100% rapid recovery.
Misinformation about heat stroke and heat exhaustion is prevalent and is seen daily on social media during the summer. One common example of this is the "red/orange man" which contains several misleading statements. Some important heat stroke mythbusters:
-Findings of skin moisture, temperature, flushing or pulse pressure are NOT essential parts of the diagnosis of heat stroke. Altered mental status is the most important finding! Oral, tympanic, temporal or axillary temperatures can be dangerously misleading. In suspected heat stroke, take a rectal temperature or treat empirically with aggressive cooling.
- Concerns of shivering, shock or hypothermia from aggressive cooling are overstated. Aggressive cooling is the best care and life-saving.
-IV fluids should not be a treatment priority. Using as much surface area as possible to rapidly cool the patient is ideal. Most heat stroke patients are euvolumic and vasoconstriction with cooling will correct relative hypovolemia. If seizures occur during cooling, consider intrasmusclar medications.
-Recognize heat stroke by considering the diagnosis in any patient presenting with CNS dysfunction during heat stress. Presentations include collapse, ataxia, agitation, and confusion. Confirm the diagnosis with a rectal temperature. Treat heat stroke with aggressive, whole body cooling.
-To prevent heat stroke, make smart decisions about the timing, duration and intensity of activity during heat and give the body time to acclimate. Drink whenever thirsty and avoid the worst heat of the day.
Twenty-one runners die in sudden cold weather exposure during 100k ultramarathon in China.
Janet T. Peterson, DrPH, WEMT, FACSM
Written on May 27, 2021

Source: The Guardian
Twenty-one runners lost their lives due to exposure and hypothermia during the Yellow River Stone Forest Ultramarathon in the Gansu Province in Northwest China on Saturday, May 22. Eight other racers were hospitalized with minor injuries and currently in stable condition. Among the dead were some of China’s top ultra-endurance athletes.
Weather turns for the worst.
The 172 ultramarathon runners who toed the line at 09:00 in fair weather for the 100K mountain trail run were unaware of the rapidly changing weather conditions in the higher elevation sections of the course. The runners, as is typical for ultraruns, were wearing lightweight clothing and equipped with a few snacks, water and the minimal required equipment- enough to see them through to the next aid station. The race course crossed into higher elevations between the second and third checkpoints, between mile 15 (24 km) and mile 22 (36 km) which included 3280 feet (1000m) of elevation gain. Most racers were in this segment of the course in the early afternoon when the weather started to change rapidly with hail, strong winds and below-freezing temperatures. Many racers were caught off guard by the weather- succumbing to the cold or falling into deep canyons while looking for shelter.
Race organizers unaware of weather changes.
Race organizers, Gansu Shengjing Sports Culture Development Co, claimed that they were unaware of the potential for extreme weather. However, the National Early Warning Information Centre meteorological service based in nearby Baiyin reported several days before the race the possibility of freezing temperatures, high winds and hail. After initial reports of lost and injured racers, organizers officially cancelled the race by 14:00 that afternoon- approximately five hours after the start of the race.
Estimated 1200 Search and Rescuers.
Initial rescue efforts were aided by less injured racers, local villagers on motorcycles and even a shepherd who was able to shelter several racers. By that evening a search and rescue team as large as 1200 was mobilized to locate and evacuate the field of racers including the use of drones and thermal imaging software. By Sunday evening the entire field of runners was accounted for, including 21 deaths and 8 hospitalized.
Race Organizers required minimal gear for runners.
According to running blog Irunfar.com and the official race website, race organizers required runners to carry the following equipment: race bib, timing chip, GPX file with route, GPS tracker, headlamp, one liter of water, whistle, emergency blanket and cell phone. First person accounts indicated that that the emergency blankets shredded in the wind and many racers became lost in poor visibility weather conditions despite GPS trackers. Jackets and other warm gear were recommended, but not required. The area is known for rapid weather changes and many have argued the runners were largely unprepared. Ultramarathon mountain running is relatively new to China and some have argued that race organizers were not as thorough or experienced in their preparations for this race.
Runner Safety First.
Organizing and executing an ultrarun is not easy in the best of circumstances. Paul Charteris, race director and founder for New Zealand’s well-known Tarawera Ultramarathon, provides insight into the myriad of factors to consider when hosting an ultra-marathon with runner safety being the highest priority including a medical director and medical safety team. The provincial government has launched an investigation to better understand the events of the Yellow River Stone Forest Ultramarathon. Although deaths during long-distance races due to both medical and environmental factors have been reported before, this has been the deadliest event to date.
Ultra-Runners at increased risk for hypothermia
A 2012 report by the American College of Sports Medicine states hypothermia is common in ultramarathoners and risk is increased in courses that are associated with water immersion, running at night, and higher elevations. Rapid changes in weather and runner inexperience were also cited as important factors. Ultramarathoners have been reported to have lower percent body fat and lower body mass index, when compared with standard marathon runners, placing them at higher risk for hypothermia. For further reading, Knechtle and Nikolaidis provide a comprehensive review on the physiology of ultra-runners and the associated medical risks.
https://en.wikipedia.org/wiki/Gansu_ultramarathon_disaster#/media/File:Gansu_ultramarathon_disaster_location_en.svg
https://en.wikipedia.org/wiki/Gansu_ultramarathon_disaster#/media/File:Gansu_Baiyin_Ultramarathon_2021.svg

http://www.time-weekly.com/post/281314
Olympic-hopeful, Katherine Diaz Hernandez, killed in lightning strike while surfing in Ecuador
By Elaine Yu, MD, MS, FAWM
Written on March 31, 2021

Source: SurferToday
Twenty-two-year-old surfer Katherine Diaz Hernandez was killed by a lightning strike while surfing at El Tunco beach in El Salvador on Friday, March 19th. She was training for the ISA World Surfing Games, the final qualifying event for the 2021 Tokyo Olympics. Hernandez was surfing with a friend and her uncle, Beto Diaz, who witnessed the event and reported that she “died instantly” after the strike. EMS providers attempted to revive her on the beach but were unsuccessful. The lightning strike was a result of a sudden weather change that turned into an unexpected storm.
Any person who is outdoors during a lightning storm is at risk of being struck by lightning. Rapid changes in weather conditions with no accessible shelter creates a dangerous environment in which people are exposed to lightning strikes on water or the ground. Surfers and boaters on open water are especially vulnerable, as in Hernandez’s case. Coastal water and beaches are more prone to lightning strikes than farther out at sea as warm updrafts when ocean air hits land are a recipe for lighting strikes.
According to the National Weather Service, 418 people were killed by lightning strikes in the U.S. from 2006-2019. Forty of those cases were attributed to fishing, 25 cases were on beaches, and 18 cases occurred while boating. The surf on a beach or the motor of a boat may mask the sound of a developing thunderstorm, putting those participating in water activities at higher risk. When lightning strikes water, it spreads out rapidly across the surface of the water, which acts a natural conductor (especially saltwater).
According to the WMS Practice Guidelines for Preventing and Treating Lightning Injuries, any time thunder can be heard, one should immediately seek shelter and wait until 30 minutes until after the last thunderclap before emerging (Grade 1C). If one cannot find shelter, they should assume lightning position (crouching with feet touching) on a non-conductive surface (pack, surfboard, sleeping pad) and avoid contact with water if at all possible (Grade 2C). If on open water, one should move to shore and away from the water’s edge or seek shelter below deck if on a boat (Grade 1C).
A victim of a lightning strike is most likely to die from simultaneous cardiac and respiratory arrest. Immediate CPR and ventilatory support should be initiated, and in a mass casualty incident these patients should be attended to first (Grade 1B). Transient paralysis is common after a lightning strike but underlying trauma and spinal injury should be considered (Grade 1C). All lightning strike victims should be immediately evacuated to the closest hospital.
Ski Lift Accidents
By Brice Rivera, Advanced Tactical Paramedic, and Phillip Griffith, MD
Posted on February 29, 2020
A New Jersey man died from an unusual ski lift accident on February 14 in Vail Colorado, which was the 6th outdoor related death in Colorado that week.
Reports say that Jason Varnish, 46, fell through an open chairlift seat. His coat wrapped around his head and neck, occluding his airway and strangling him. He was pronounced dead at a local hospital, and the Eagle County Coroner's office concluded he died from positional asphyxia.
Ski lift accidents are exceedingly rare. Prior to February 14, the last American ski lift fatality was in December 2016, when a woman and her children were thrown from their chair after it slammed into a lift tower due to a drivetrain malfunction.
According to the National Ski Areas Association, a person is five times more likely to die riding an elevator than a ski lift. Additionally, most American skiing fatalities are from direct collisions, with 42 skiing related deaths in the 2018/2019 season, and 95% of all deaths being males. However, this does not include medical related deaths and deaths outside of ski-resorts.
Five other outdoor related deaths occurred the same week in Colorado, including:
- Two men who died in a snow-bike related avalanche.
- A skiing accident involving a 70-year-old man who struck a tree.
- A skiing accident involving an 83-year-old man who fell off a half-pipe
- A 77-year-old woman who went missing while Nordic skiing.
The most deadly ski lift accident in history was the 1976 Cavalese Cable Car disaster, when the steel cable broke as the car was descending. It fell 200 meters, killing 42 people with one survivor. In 1998, at the same site, a US Marine Corps Prowler jet struck and severed the cable of the aerial lift, killing 20 people and causing an international incident.
According to Medscape, most strangulation deaths are due to suicide, assault, or accidents. While the pathophysiology of strangulation is controversial, with the exception of judicial hangings in which the mechanism is essentially decapitation, the main causes of death from strangulation are attributed to venous obstruction, arterial spasm, or vagal collapse. These pathways all converge to hypoxia, ischemia, and death.
These mechanisms differ from judicial hangings, where the victim drops from at least their height. In a judicial hanging, the victim dies from internal decapitation, which fractures the cervical spine, transects the spinal cord, and distracts the head from the neck. Death is usually instant.
Suspension syndrome ("Harness hang syndrome") is another hanging related injury. In suspension syndrome, a hanging patient has decreased venous return from being upright. Eventually, the decreased venous return causes the patient to syncopize and collapse, which when the patient is prone, causes an increase in venous return. Unlike syncope on the ground, the patient does not fall and there is no improvement in venous return resulting in decreased blood flow to vital organs. Eventually, death occurs from shock or hypoxia.
Ski resorts are generally known to be relatively safe for all experience levels, whether one is carving down the bunny slope, black diamond, or even cross country skiing the backcountry. Nevertheless, there's always a potential for risk, especially in colder climates, even for the most experienced outdoorsmen. The American Academy of Orthopedic Surgeons cites data that in 2018, nearly 200,000 emergency room visits were from preventable injuries resulting from individuals participating in winter sports.
Risk mitigation is key to keeping you safe outside. Consider attending the WMS Winter Conference in Sun Valley February 29-March 4 to learn more on these important topics. Practicing these essential tips can help you prevent injuries.
- Learn proper technique. If it's your first time on skis or a snowboard, taking lessons will help ensure your safety when navigating terrain.
- Know your gear. Always inspect your equipment and that it functions properly. You don't want a malfunction when you're bombing down the mountain. Helmets and goggles with UV protection are a few protective items that are ideal to have on your person.
- Wear protective clothing. This involves a combination of loose moisture-wicking water and wind-resistant outer shells.
- Know the environment. Taking note of the weather forecast and your fluctuating body temperature during high, moderate, and low activity levels will help tailor what you need to prevent cold-related injuries like frostbite or hypothermia through adequate body temperature management.
- The Wilderness Medical Society Clinical Practice Guidelines can provide further information on hypothermia and frostbite, and the management of other cold-related injuries.
- Prepare for the worst. For example, when going into avalanche country, make sure you have a working avalanche beacon, shovel, and probe. Carry more food than you think you will need. Have a first aid kit, know both what's in it and how to use it.
- Make a plan and share it. Ensure someone knows where you are going and that you have a way to contact someone should something happen. While cell phones don't always work in remote areas, satellite communication devices, such as a Spot or Garmin Inreach will provide a means of communication.
- Know yourself. Be mindful of your own limitations.
- Properly warm up. Cold muscles and tendons are prone to injury when just starting outdoor sports.

Ski Lifts on Mt. Tremblant (flickr.com/photos/7617731@N02/3891290898)
Bear attack reported near downtown Aspen, CO - by Mary Rosegrant, DO
Posted on May 31, 2019
Earlier this week, Colorado Parks and Wildlife began the search for a black bear that attacked a woman while she and her husband were hiking along the Hunter Creek Trail a heavily-trafficked, 1.5 mile, downtown Aspen trail.
While walking along the path, the couple noticed the bear approaching. They stepped to the side of the trail to allow the bear to pass when it turned toward the woman and bit her in the thigh before running off. The attack was reportedly "out of the blue," though the hikers admitted to having stood quietly along the trail without making loud noises or attempting to make their presence known.

Though injuries were minor two puncture wounds at the bite site the attack is considered aggressive as it was unprovoked and near a well-populated area, so the bear believed to be responsible was tracked down by Colorado wildlife officials and was killed. Authorities searching for the animal believed it was a young black bear, about 2 years old, and are awaiting DNA test results to confirm it's the correct bear.
Bear attacks are rare with only about 177 attacks reportedly causing injury or death in North America since 1955 (see WMS link below). However, many have been killed in Colorado alone due to behaviors considered to be threatening to humans, such as entering homes in search of food.
Though many of these encounters have not involved overt attacks or aggression toward humans, the approach is one of prevention. In some cases, relocation after exposure to humans is attempted, though it is often unsuccessful as bears become unafraid of humans and can become aggressive without warning. In 2017, Colorado reported euthanasia of 216 bears and relocation of 109.

Tips for bear encounters:
- DO NOT run from the bear; this could trigger a chasing response and provoke an attack
- DO NOT climb a tree
- DO NOT drop your pack or offer food
- DO stand tall with your arms raised high, make yourself appear large, and talk loudly and firmly
- If noticed by a bear at a distance, walk slowly and sideways in the opposite direction
- If you notice a bear but it has not noticed you, DO NOT shout/startle the bear as it may provoke a defensive response
- If the bear exhibits defensive behavior (huffing, clicking teeth, moaning, striking the ground/tree, bluff charging), raise your arms and speak loudly, but try not to appear threatening
- If attacked as prey, look as large as possible and shout; fight back using any weapons found (rocks, sticks); aim at the eyes, nose, and face
- This response is most typically appropriate for attacks by blacks bears
- If attacked defensively, lie prone on the ground, cover your neck with your arms, and spread your legs to prevent being flipped over; always return to a prone position if rolled; do not fight
- This response is most typically appropriate for attacks by grizzly bears
- Carry bear spray in areas with known black or grizzly bears; it has proven most effective in deterring aggressive attacks (see the video below)