I had been recently invited on a 16-day whitewater rafting trip down the Grand Canyon, a remote 230-mile section of the Colorado River. As an Emergency Medicine senior resident, I took charge of organizing the medical aspects of our trip. I was no stranger to planning wilderness adventures, however, the remoteness, extreme environment, and large group size presented new challenges. Additionally, with the growth of my medical knowledge came a “standard of care creep” for the level of care I expected myself to provide.
I pondered what to bring—what antibiotics provide the best coverage? How to acquire prescription travel medications? When to suture a wound in the backcountry? How many EpiPens to bring? Should we bring IV fluids? Seeking an evidence-based approach, I reviewed current literature and practice guidelines to build an evidence-informed expedition medical kit. With this resource, I hope to offer a framework for future trip leaders to elevate the medical care of their wilderness trips.

Will it fit? (created by leonardo-ai)
Environmental and Group Factors
Serious medical incidents requiring evacuation are uncommon, however, even minor incidents can present a significant risk and burden on the group. Understanding the group’s pre-existing risk factors is the first step towards medical preparedness. Review group-member medical conditions, allergies, and medications. Ensure those with chronic conditions plan with their specialist and bring sufficient medication.
Consider specific hazards presented by local terrain and environment. What weather and temperature are expected? Altitude? Hazardous plants/animals? Identify potential evacuation routes by foot, litter, or helicopter. Review emergency communication availability with cell signal or GPS devices like satellite phones. Identify contact for local rescue service.
Medical Kit Basics
Med kits should be tailored to each expedition and balance comprehensiveness, versatility, medical training, group size, weight, and cost. Ensure the container is sturdy, easily accessible, and protected from the environment. Items should be clearly labeled. All group members should be aware of kit location and content.1

Ammo can med kits for the Grand Canyon (Canyonlands Field Institute)
Obtaining Medications and Supplies
Most medications can be purchased over-the-counter. Obtaining prescription medications for travel can be challenging. One option is for each group member to obtain personal prescriptions after consultation with their doctor or travel clinic (in some US states and countries, pharmacists can prescribe certain medications). Alternatively, for prescriptions for group use, Moore et al. outline a guideline for prescribing medications for expeditions. During a pre-trip consultation, the necessary medications are prescribed to the trip leader for group use with appropriate medication administration training. If possible during the expedition, a telehealth consultation would be performed prior to medication administration. If not feasible due to austere environment, clear written instructions for emergency use are provided.
Specialized medical supplies like tourniquets can be purchased from pharmacies or online suppliers. Some supplies like suture or lidocaine may require a physician medical license and bulk ordering. Take caution when traveling, especially internationally. Ensure are medications are clearly labeled and prescribed to the carrier. Refer to the International Narcotics Control Board for specifics on traveling with controlled substances.
Medical Literature Recommendations
IV Access:
- IV medications/fluids: Challenges are posed by sterility/infection risk, patient environmental exposure, and provider needlestick risk. Tactical Combat Casualty Care guidelines recommend considering wilderness IV access only for patients in acute hemorrhagic shock or who require an IV medication. However, most essential medications have equally efficacious alternative routes. Consider IV access if in a basecamp setting or anticipate significant delayed rescue.1
Airway Emergency:
Cardiac arrest:
Major Hemorrhage/Trauma:
Anaphylaxis:
- Epinephrine (1:1000) IM: First-line for treatment of anaphylaxis. Autoinjector devices are convenient but costly. Multiuse vials are more cost-effective, though carry possible increased risk of needlestick injury, delayed administration, and dosing errors. Epinephrine should be stored at 20-25 °C, however, for wilderness temperatures there has been no effect seen on drug efficacy with freezing, and heat likely only has modest effect. Discolored or expired epinephrine may be less effective and recommend against usage, however, several studies showed retained efficacy for up to 24 months past expiration. Recommend access to multiple doses. Upwards of 8-17% of patients will require multiple doses of epinephrine, with 2.2% requiring 3 or more doses. EpiPens are designed for single use, however, disassembly of autoinjectors to obtain additional doses in case of persistent anaphylaxis symptoms has been described.
Analgesia:
Wound care:
- Abscess: Consider incision and drainage kit with scalpel, irrigation, and vessel loop.2 If no surrounding cellulitis, no indication for antibiotics after I&D.
- Irrigation: Use any potable water. Can use syringe and needle for pressure irrigation. Avoid soap or antiseptics as these lead to impaired wound healing.
- Wound Closure: Sterility is impossible in wilderness conditions; however, primary repair improves function, cosmetic outcome and healing time. Grossly contaminated wounds should be packed open with wet to dry dressing to heal by secondary intention or delayed closure. Most other wounds can be safely closed with suture or stables. For low tension wounds, consider tissue glue or steri-strips. See wound prophylaxis below.
Infection:
- Work with a travel medicine doctor or pharmacist to select the most appropriate antibiotic coverage per local resistance patterns.
- Soft tissue: Cephalexin covers most skin flora. Agents like trimethoprim-sulfamethoxazole, doxycycline, or clindamycin include additional MRSA coverage. No significant difference in outcomes has been found between agents. Doxycycline carries significant risk of photosensitivity, an important concern for the wilderness setting.
- GU: Antibiotics such cefalexin, ciprofloxacin, doxycycline, nitrofurantoin, trimethoprim-sulfamethoxazole provide good coverage for common urinary pathogens.
- GI: First line treatment excellent hand hygiene, hydration, and symptomatic management. Most acute diarrheal infections ≥80%–90% are bacterial. However, empiric treatment with antibiotics is not recommended unless the patient is high risk (e.g. immunocompromised) due to risks of adverse effects, gut microbiome disruption, and resistance. If utilized, recommend rifaximin/rifamycin or azithromycin, due to higher adverse effects and resistance with fluroquinolones.
- Pneumonia: Amoxicillin and doxycycline have good coverage for respiratory pathogens for low-risk patients.
- Wound prophylaxis: Recommend for contaminated wounds, bite wounds, involvement of deeper structures (bone, joint, cartilage, tendon) with amoxicillin-clavulanate, second generation cephalosporin, or doxycycline.1 Consider need for tetanus or rabies prophylaxis.
Ocular Complaints:
- Corneal abrasion: Can identify corneal defects using fluorescein stain and a penlight with blue light filter. “Cobalt blue light” apps for smartphones are also available. Prophylaxis with erythromycin ointment or moxifloxacin ointment if contact lens wearer.
Urologic Emergencies:
- Urinary retention: Consider 18F coudé foley catheter for acute retention. If unavailable, emergent suprapubic decompression can be performed with a needle and syringe.
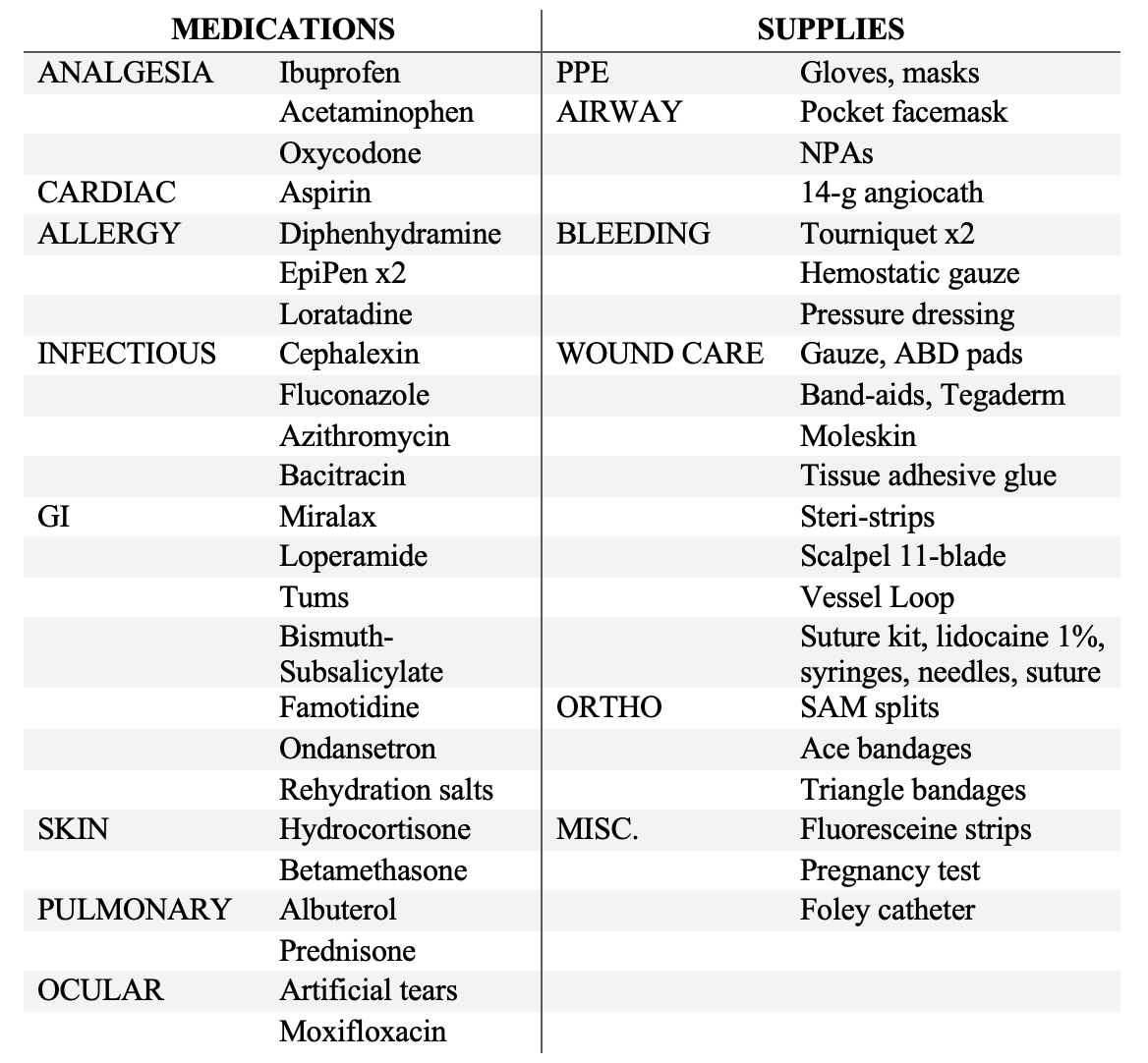
Sample Medical Kit
Additional Textbook References:
2. Auerbach PS, Cushing TA, N Stuart Harris. Auerbach’s Wilderness Medicine. Elsevier; 2016.
1. Bledsoe GH, Manyak MJ, Townes WA. Expedition & Wilderness Medicine. New York, New York: Cambridge University Press, 2009.