On Sunday, May 17th, a hiker fell into a deep rock crevice roughly 400 feet from the entrance of Merlin’s Cave in New York. The victim’s companions descended into the crevice to assist, maintaining great efforts to keep the patient warm and calm under this extreme circumstance. Utilizing a hammer found inside the cave, the friends even managed to manually chip away a portion of the restricting rock before professional rescuers arrived.

Hiker wedged in cave. Source: New York State Department of Conservation
The Albany Schoharie Cave Rescue team was mobilized later that evening. Forest Ranger Lieutenant John Gullen noted that the primary hiker was tightly molded into the structural contours of the crevice, having been wedged fast for over six hours. Rescuers utilized hammer drilling to chip away the restricting rock formation, successfully freeing the primary victim within 20 minutes of reaching him. Rescuers and the victims then shimmied through the narrow passages to reach the surface, concluding this high-stakes rescue mission.
Merlin’s Cave sits at a baseline ambient temperature of approximately 50 degrees Fahrenheit with 100% relative humidity, making it a perfect setting to develop hypothermia. High humidity accelerates evaporative cooling while simultaneously saturating clothing, effectively destroying the body’s boundary layer of insulation. While normal physiology relies heavily on radiation for heat dissipation, environmental exposure in a cave flips the script, forcing the body to lose heat rapidly via convection (moving cold air currents) and conduction (direct contact with wet mud and cold stone). When a patient is fully immersed in water or wet mud, conductive heat loss can skyrocket up to 25 times faster than in air.
Under normal circumstances, a healthy individual balances this environmental gradient by accelerating metabolic heat production by constant movement and shivering. However, when an injured caver or hiker is physically pinned or static, they cannot generate compensatory heat. Without immediate rescue and external thermal insulation, rapid progression to severe hypothermia is inevitable.
Manifestation of hypothermia depends on the core body temperature.
- A core temperature of 37-35 C: feeling cold, shivering, pallor, impairment of fine movements.
- A core temperature of 35-32 C: Uncontrolled shivering, mental slowing, memory impairment.
- A core temperature of < 32 C: Altered mental status, cessation of shivering, cardiovascular collapse, and coma.
Initially, the autonomic nervous system triggers a massive sympathetic response: shivering to generate heat, and profound peripheral vasoconstriction to protect vital organs. However, if environmental heat loss continues to outpace the body's caloric reserves, the shivering ceases. As the core drops below 32°C, multi-organ failure becomes a concern.
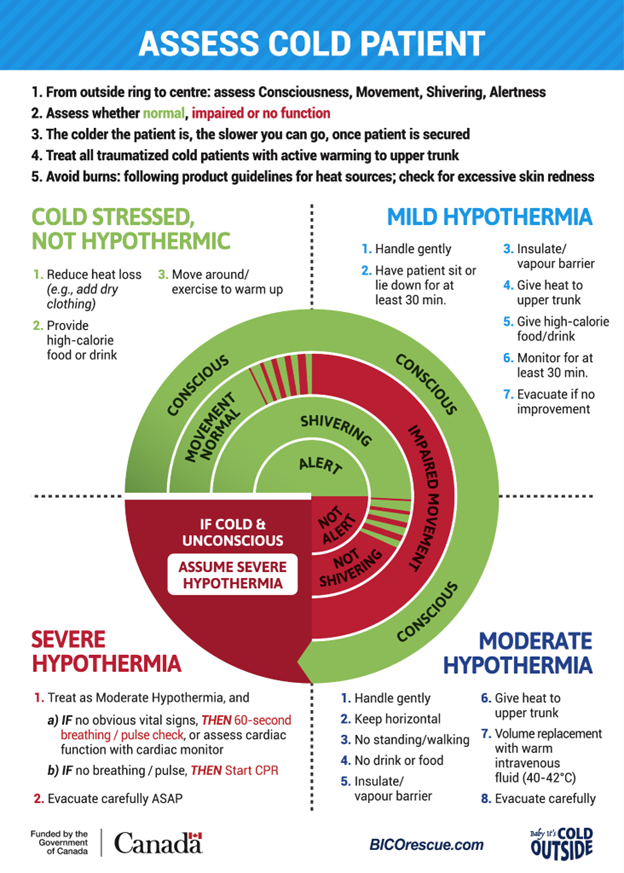
Cold Card for rescuers. Source: BICO Rescue via WMS.
It is important for injured cavers to remain dry and remove wet clothing. Initial treatment should focus on passive warming with insulating layers and prevention of heat loss with a vapor barrier. It is also recommended to give warm fluids by mouth if access if possible which helps elevate body temperature.
Sometimes access can be difficult, such as it was in the well-documented 12 hour cave rescue in Virginia. An adult male was pinned vertically within a tight rock fissure, and this confinement made providers unable to obtain baseline vital signs, place standard monitoring equipment, or establish intravenous/intraosseous access due to restriction of the patient's extremities. During this long ordeal, the patient remained alert and oriented but was slowly deteriorating due to progressive hypothermia. The rescuers tried to chemically rewarm him with wherever was accessible. The patient became lethargic with moderate shivering with some low blood pressures, but ultimately returned to baseline and vital function once he was pulled out and rescuers actively warmed him with full access.
The Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update uses a clinical staging based on level of consciousness, shivering intensity, and cardiovascular stability. Mild cases require passive insulation, removal of wet garments, recumbent positioning to optimize shivering thermogenesis, and core-targeted active warming. Moderate cases command aggressive external rewarming (axilla, chest, groin), specialized horizontal handling to prevent afterdrop arrhythmias, and volume resuscitation via IV/IO lines with warmed fluids. Severe cases necessitate advanced airway management for comatose patients, a prolonged 60-second pulse check to rule out profound bradycardia, and immediate CPR/defibrillation modification if cardiac arrest is confirmed.