Healthcare’s Hidden Carbon Burden
Globally, healthcare accounts for a substantial share of national carbon emissions, ranging from 3% in England to 10% in the United States. This 10% in the U.S. translates to 19 kg of waste per patient and 6600 metric tons of waste daily, totaling two million tons of waste annually. Within this medical system, a single emergency department can generate 672kg of waste in a 24-hour period, 2kg of total waste per encounter and translating to 3110kg of carbon emissions. While environmental waste may seem unavoidable in the context of intense, and productive emergency medicine, these emissions are substantial after they’re multiplied to over 130 million emergency visits annually, with 155 million visits in 2022. Much of this waste comes from single-use plastic, including materials for one of the most routine procedures in the ED: peripheral intravenous (PIV) access.
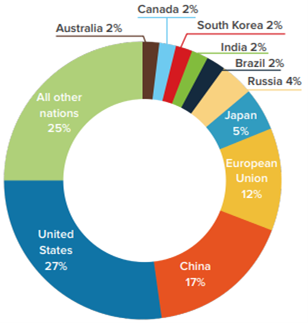
Top ten emitters as percentage of global healthcare footprint (2019 Health Care Without Harm foundational analysis, Health Care’s Climate Footprint)
PIV placement is foundational to emergency medicine. A peripheral intravenous catheter is a small plastic tube inserted into a vein, typically in the arm, and provides a route for administration of fluids, medications, blood products, and contrast agents, along with diagnostic testing. Between 60-70% of patients in the ED receive a PIV. The unpredictable nature of the emergency department has motivated clinicians to act proactively, rather than reactively. A “just in case,” however, is not without consequences.
Placed but Not Used
Just because most patients have a PIV, it does not mean it is always utilized. Some studies suggest that as many as 35-50% of PIVs remain unused in some emergency departments, with up to 43% of unused PIVs remaining unused even after admission into the hospital. At the same time, PIVs placed in the field are frequently replaced, one study showed that 73.7% of lines were replaced due to hospital protocol, despite the maintenance of patency and functionality. Regarding infection rates, one study showed no clinically or statistically significant increased risk of infection between prehospital and in-hospital placed PIVs. Addressing unnecessary PIV placement and replacement requires a multifaceted approach, including development of evidence-based guidelines and implementation of improved techniques.
Guided by Habit, Not Evidence
There are currently no universally accepted guidelines that define indications for placement of PIVs. Decisions are driven by clinician judgement and institutional protocols. However, evidence suggests implementation of criteria can reduce unnecessary PIV placement. A 2014 survey generated a list of criteria to reflect “a high likelihood of requiring therapeutic interventions administered intravenously, and those at risk of sudden deterioration where an existing intravenous line would expedite intervention”. However, the study still concludes that clinician judgement drives the decision for PIV placement, given the complexity and variability in clinical presentations. Literature is still emerging, which may be useful in the development of clinical decision tools for PIV placement. Each unused catheter, each unnecessary replacement, and each repeated attempt contribute to a growing environmental burden, which can be alleviated by moving towards evidence-based standardization guidelines.
First Attempt Done Right
Importantly, implementation of ultrasound-guided PIV placement is feasible, as training can be completed using readily available resources and equipment found in most EDs without substantial time investment.
Whether the patient is receiving their first PIV or if it is being replaced, many times they require multiple attempts. On average, 1.3 to 1.74 attempts were required prior to a successful PIV insertion, with only a little more than 50% being successful in the first attempt. Progress and access to medical technological advances offer promising solutions. Ultrasound-guided PIV placement has demonstrated higher first-attempt success rates of 85.7%-90%, along with fewer complications and longer catheter dwelling times, meaning the PIV remains functional for a longer period before requiring replacement, resulting in decreasing resource use, patient discomfort, and associated waste. While the EPIC randomized trial and DIAPEDUS study which showed this increased first-attempt success rate with use of ultrasound focus on the pediatric population, the underlying principles seems likely applicable to the general population. Although research is limited in this area, a single study in an ED that cares for both children and adults showed cost reduction with ultrasound-guidance compared to traditional placement, with an increase in catheter dwell time relative to hospital length of stay. Importantly, implementation of ultrasound-guided PIV placement is feasible, as training can be completed using readily available resources and equipment found in most EDs without substantial time investment. In one study from the Department of Emergency Medicine at George Washington University Hospital, a protocol for ED technicians involved only a two-hour training session, covering the principles of ultrasonography, machine operations, US-guided venous cannulation, and upper extremity venous anatomy, suggesting that ultrasound-guided PIV training programs may be implemented without extensive additional infrastructure or prolonged training requirements while still providing an optimal patient experience. Improved first- attempt success enhances patient experience, decreases hospital costs, and reduces environmental waste from associated repeated attempts.
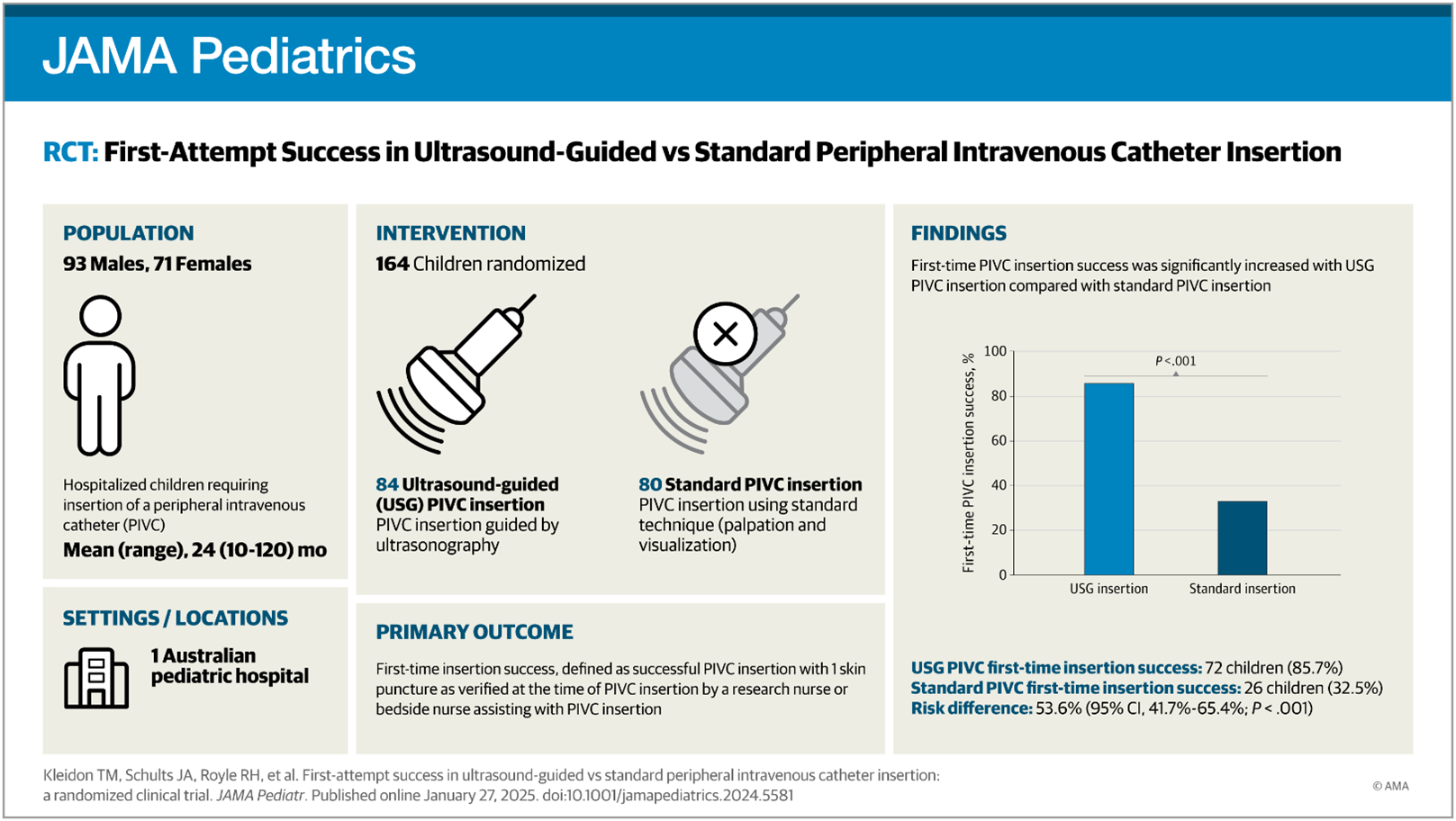
Results for the 2025 JAMA Pediatrics article, First-Attempt Success in Ultrasound-Guided vs Standard Peripheral Intravenous Catheter Insertion: The EPIC Superiority Randomized Clinical Trial
Are We Really Doing No Harm?
Every placement carries not only an environmental cost, but also a clinical one. PIV placement can be a source of pain for patients and each attempt increases the reported experience of pain. Disruption of the skin barrier during PIV placement also introduces a route for bacteria to enter the body, increasing risk for skin and bloodstream infections and thrombophlebitis. In one study, 23.5% of healthcare-associated Staphylococcus aureus bacteremia episodes were deemed PIV-associated. Among these PIV-associated episodes, 39.6% involved PIVs placed in the ED. With its high non-utilization rates and potential risks, it’s worth considering if routine PIV placement really does “no harm.”
Rethinking Routine Practice
PIV placement is fundamental in providing excellent emergency care, it’s often routine and reflexive, but carries both environmental and clinical implications. A considerable proportion of PIV are unutilized or, potentially, unnecessarily replaced due to protocol rather than clinical need. The most important first step in changing clinical workflow is the implementation of an evidence-based approach to help guide a clinician’s decision for PIV placement, such as institutional-specific pathways for management of certain clinical presentations. Local, institution-specific research can help identify and further refine the current approaches that would reduce avoidable placement, supply use, and waste, without compromising emergency care. Further broad research is needed to transform the current trend of vague clinical judgement into a validated standardized criterion. Technological advancements with improved access to ultrasound are promising ways to improve success in PIV placement, resulting in higher patient satisfaction, lower complication rates, and reducing waste with new supplies for each new attempt. Implementation of such strategies would likely include protected training time, and continued education credits for clinicians and other non-monetary incentives to encourage the adoption of ultrasound-guided techniques. It is possible to decrease environmental impact without compromising clinical outcomes.
In a generation where climate awareness is at the forefront of everyone’s mind, even the most standard and routine medical dogma deserves reexamination. The peripheral intravenous line, often overlooked, offers an impactful opportunity to align clinical practice, patient-centered care, and environmental responsibility.