One of the classic definitions of wilderness medicine that we teach in WFR and WALS courses: it is medicine practiced in a context where resources are limited and transport to definitive care is significantly delayed. Traditionally, we associate this with the High Sierras, a remote canyon in Utah, or a trawler off the Atlantic coast. We define the "wilderness" by the miles we must traverse to reach help.
But what happens when the miles stay the same, but the help disappears?
In the state of Maine, we are currently witnessing a disturbing shift that challenges the geographical definition of our field. Through a combination of hospital unit closures, loss of trauma accreditations, and a swelling population, the resources of the "front country" are shrinking to match more of our typical expectations for an austere environment. As emergency physicians and EMS providers, we are finding that many of the principles of wilderness medicine—prolonged field care, resource improvisation, and managing deterioration over time—are no longer just for the backcountry. They are becoming a necessity even within our towns and cities.
The Shrinking Map of Definitive Care
The cornerstone of modern trauma systems is the "Golden Hour"—the idea that rapid transport to a specialized center saves lives. In Maine, that safety net is fraying.
Perhaps the most striking example is the recent shift at Central Maine Medical Center (CMMC). Historically a pillar of trauma care in Lewiston, CMMC’s decision to relinquish its trauma accreditation fundamentally alters the triage map for a massive swath of the state. For a paramedic responding to a multi-system trauma in a town that was once 20 minutes from definitive stabilization, the drive might now be an hour or more to the next Level 1 or Level 2 facility.
This is no longer a "scoop and run" scenario; it is a prolonged transport requiring the management of coagulopathy, hypothermia, and hemodynamics over distance—skills typically managed over short intervals, now requiring forward thinking classically reserved for critical care transport or advanced wilderness rescue teams facing prolonged extrication.

The "Golden Hour" becomes the "Golden Afternoon": EMS crews in rural Maine must now manage critical trauma patients over significantly longer distances and through challenging conditions as central resources consolidate. (Image Credit: Sigmund via Unsplash).
Simultaneously, we are watching a slow-motion collapse of obstetric infrastructure. The closure of the birthing center at Northern Light Inland Hospital in Waterville is not an isolated event; it is part of a contagion of closures across the state. We have seen Labor and Delivery units shutter from Bridgton to Rumford, creating massive "OB Deserts."
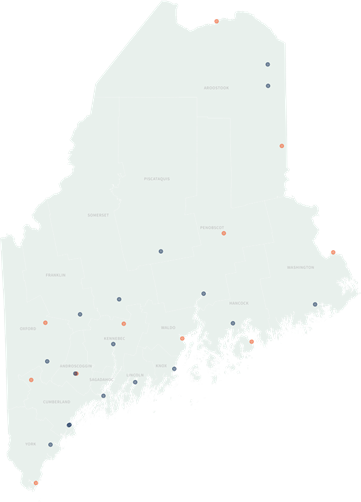
A visual representation of the "maternity desert" growing in Maine. This map details the closure of obstetric units across the state, forcing rural patients to travel significantly further for definitive care. Orange represents a closed unit. Blue represents an operational unit. (Image Credit: The Maine Monitor, used for educational commentary).
When a precipitous delivery or an obstetrical emergency occurs in these regions, the "local" ER may no longer have the equipment or the specialist staffing to manage it. The EMS crew or the rural ED physician are effectively operating in a resource limited environment , managing a high-risk delivery with limited backup, knowing that the NICU is two counties away.
The Population Press
While the medical infrastructure contracts, the demand is doing the exact opposite. Maine has seen a significant influx of new residents, driven by pandemic-era migration and climate migration trends. We are seeing an increasing state population that is effectively stressing a shrinking system. At the same time, hospitals are seeing less and less stable funding both at a state and federal level and from dwindling payments from private insurance companies. Most hospitals also face significant recruitment issues as healthcare professionals preferentially have gravitated to urban centers.
This inverse ratio—more people, fewer resources—creates a bottleneck. It is not uncommon now for ambulances to be "held on the wall" at emergency departments for hours due to overcrowding or for inter-facility transfers to be delayed by days due to a lack of ICU beds.
When a patient is stuck in a rural ED for 36 hours waiting for a transfer, or when an ambulance is the only medical asset available for a patient for a two-hour transport, we begin to dip into management concepts and education most commonly seen in Prolonged Field Care (PFC). The mindset required to manage that patient parallels the mindset required to manage a climber with a broken femur awaiting a helicopter rescue. We must monitor trends, manage physiology, and anticipate problems long before they happen, because the cavalry isn’t coming quickly.
Adapting the Wilderness Mindset
So, what does this mean for the wilderness medicine practitioner? It means our skills are more relevant than ever, but the context has expanded.
- Reframing "Wilderness": We need to stop thinking of “wilderness” medicine as something that only happens in the woods. A rural ED with no blood bank and no surgeon functions similarly to a wilderness environment. We must maximize what we can do in a resource limited setting and rapidly transfer the patient to appropriate care – concepts heavily emphasized in wilderness medicine. An ambulance on a 90-minute divert to a tertiary center must prioritize and even improvise, transferable skills from wilderness medicine training.
- Training for Time: EMS and rural hospital education must pivot to emphasize the "middle game." We are great at the first 15 minutes of resuscitation. We need to get better at hours 2, 3, and 4. How to do this will be multi-factorial but one proposition is to carry some wilderness medicine topics into this sort of training. Namely, our wilderness medicine tendency to keep things simple can help tremendously in this situation. We train ourselves to address minor problems to keep them from causing significant downstream impacts. Blisters on our feet? We address them with better equipment or wound care before they can sabotage our expedition. Only two rescuers on scene with many tasks needing completion? Lacking in the right supply but still needing it done? We have many transferable skills to offer aid as the availability of our resources shrink.
- Community Integration: Just as a wilderness expedition plans for evacuation routes, our communities need to plan for these gaps. This means more robust community paramedicine programs to catch issues before they become emergencies, effectively triaging the "expedition members" (our citizens) before they need a rescue.
The line between the "street" and the "wild" is blurring. As resources retreat, the wilderness is reclaiming the map, not with trees and rocks, but with time and distance. For the providers in Maine, the challenge is clear: we must apply the improvisation, resilience, and clinical acumen of the wilderness physician to the paved roads of our own towns.