
Rescuers prepare to search for missing avalanche victims. Source: Nevada County Sheriff’s Office
“Big storm incoming! Use extra caution this week!” posted Blackbird Mountain Guides, a Pacific Northwest-based guiding company. Forty-eight hours later, on the morning of February 17th, 2026, at approximately 11:30 AM, 11 clients and four guides from the company were involved in the deadliest US avalanche incident since 1981. The individuals were returning from a three-day expedition to the remote Frog Lake Backcountry Huts located near Castle Peak, an area deep in the Tahoe National Forest wilderness which sees an average of 35 feet of snow a year, when the D2.5 avalanche struck.
Placer County Sheriff’s Office reported roughly 50 search and rescue members deployed and by 5:30 PM successfully located and rescued six survivors, five clients and one guide, whom all sustained non-life-threatening injuries. As of February 19th, harsh conditions continue to hamper recovery of the remaining nine individuals, eight of whom are confirmed deceased while the ninth person has not been located, but is presumed deceased. This tragedy marks the second fatal avalanche incident in the region this year following the death of a snowmobiler on January 6th, 2026.
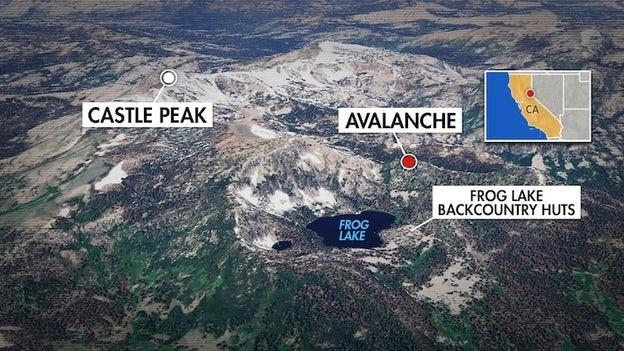
Key locations in one of the deadliest avalanches in US history. Source: Fox Weather
Each winter, 25 to 30 people die in avalanches in the US, making them the deadliest natural hazards on National Forest public lands. Morbidity and mortality largely depend on the degree of head and chest burial, duration and depth of burial, and access to oxygen, with asphyxia driving roughly 75% of fatalities. Proposed mechanisms for asphyxia include airway obstruction, hypercapnia, progressive hypoxia from rebreathing expired air in a small air pocket, and external chest wall compression from dense snowpack impairing ventilation. Fatalities secondary to hypothermia are uncommon due to the asphyxia’s rapidity of onset. Mainstays of avalanche morbidity and mortality prevention thus center on strategies to avoid being caught in an avalanche, avoiding critical burial, and avoiding asphyxiation if buried.
To avoid being caught in a slide, key cornerstones of avalanche risk mitigation include avoiding travel during and immediately after heavy snowfall, significant winds, and rapidly changing temperatures. The Sierra Avalanche Center forecasted a high chance of life-threatening avalanches in the region during the time of the incident. During such advisories, travel in avalanche terrain is not advised. If travel is necessary, spreading out is critical to avoid multiple people getting caught in a slide. Secondary analysis has indicated that the group likely had been caught while transitioning, and therefore were not spaced apart. Additionally, they were in relatively low-lying terrain and likely did not anticipate that propagation would reach them were a storm slab to release from above. It is suspected that difficulty with parking and getting permits for such a large group likely led to the group choosing a higher avalanche risk egress route compared to the longer, but recommended exit route during a storm.
This D2.5 avalanche (large enough to bury a person, car, or house) was likely a large storm slab that had recently settled on highly unstable facets from a recent dry spell. With the continued storm, new snow has settled on that layer and continues to pose extremely high avalanche risk. While the survivors were evacuated, the bodies of the deceased have yet to be extricated amidst ongoing avalanche danger.
If unable to escape sliding snow, strategies to avoid burial and mitigate asphyxia include using swimming motions to stay on the surface, covering the mouth and nose with the crook of your elbow, removing skis or snowboards, and ensuring you are equipped with an avalanche airbag. Use of these inflatable backpacks or vests can reduce mortality rates from 22% to 11% by reducing incidence of critical burial (defined as head and chest below the snow) and increasing the size of life-saving air pockets if critically buried. All travelers in avalanche terrain should also be equipped with beacons which have been shown to reduce the time between critical burial and rescue, from 102 minutes to 20 minutes ultimately increasing chances of survival.
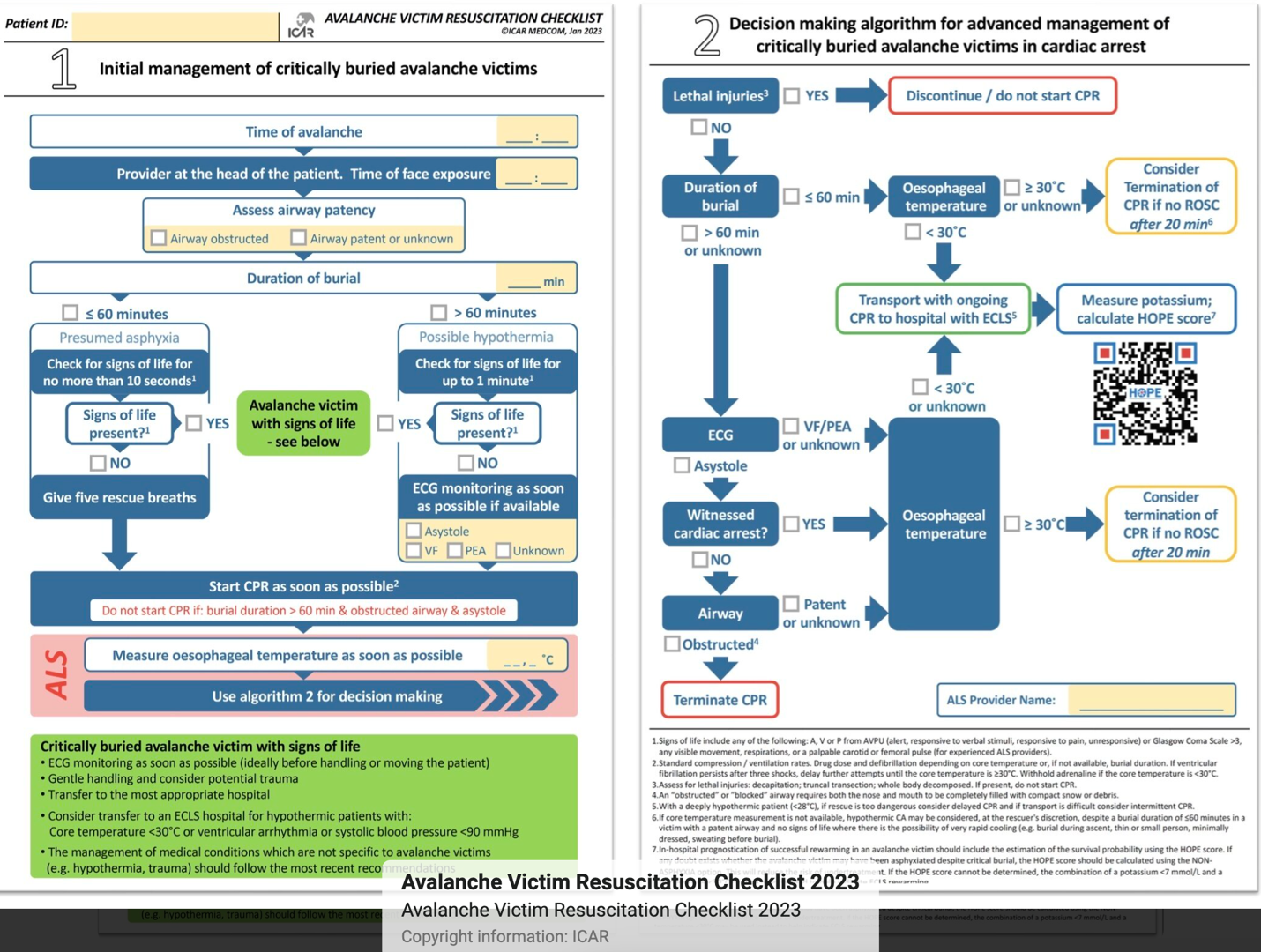
Proposed approach to avalanche rescue underscoring importance of airway patency, duration of burial and core temperature. Source: International Commission for Alpine Rescue
This tragedy also highlights many unique aspects of mass casualty avalanche events. Use of specialized triage systems, such as the AvSORT algorithm, can improve victim outcomes by prioritizing prompt victim extrication, noting survival rates of victims plummets from 92% at 15 minutes of burial time to only 30% at 35 minutes. These algorithms also place strategic emphasis on key survival factors such as patency of airway, size of air pocket, relative burial depth (80% probability of survival at burial depth less than 50 cm compared to only 10% at greater than 200 cm) and core temperature at extrication (victims found pulseless and apneic with core temperature > 30 C have most likely died from asphyxia). In addition to these complicated tactical triage nuances, rescuers are often also hindered by ongoing environmental hazards such as additional avalanches, inclement weather and health risks such as hypothermia, frostbite and exhaustion.
Stress continuum for patrollers. Source: Ski Area Management Info
Before, during, and after a large search and rescue operation, many organizations utilize tools like the stress continuum to assess in real-time the readiness of individuals or an entire team. Critical Incident Stress Management (CISM) is a crisis intervention system that helps supports groups and communities throughout an incident to mitigate long-lasting psychological effects after an incident. Debriefing stages are predefined and designed to help return an individual/team back to fully functioning. The stages of CISM debriefing are:
- Assessment phase – understand needs of the group
- Fact Phase – describe facts surrounding the incident
- Thought phase – share thoughts/feelings surrounding the incident
- Reaction phase – discuss impact on individuals
- Symptom phase – share physical/emotional symptoms
- Teaching phase – understand/normalize reactions to stressful incidents
- Reentry phase – synthesize information gathered/learned and focus on healthy coping mechanisms and readiness for the next incident