The television was replaying Arizona’s Final Four loss when my pager erupted.
“Cave rescue.”
My wife and I exchanged the look that comes with decades in wilderness medicine. This would not be quick. Possibly all night. We moved through the familiar choreography—cave pack, frozen water bottles, redundant headlamps, and batteries in quantities that would embarrass a small electronics store. Underground, light is not merely helpful. It is survival equipment.
Radio traffic filled in the outline. An experienced caver had fallen. She was conscious, alert, and in severe back pain. By the time we had traveled the 60-odd miles to the remote site, one of our team was already with her. At base camp I scanned the hillside for the cave entrance and saw nothing but brush and shadow. In southern Arizona, caves have a way of pretending not to exist.
“You’ll stay at the entrance to communicate,” someone said as we climbed.
“How much farther?” I asked.
“Not far,” they said—using the definition of distance that all wilderness rescues routinely falsify.
The entrance was just a slit in the rock. The plan was for me to evaluate the patient by cave phone—an old, wired device that looks better suited for transmitting troop movements than vital signs. The technical team had other ideas.
“We need you with the patient.”
I paused. “I’m going in?”
They nodded. The ropes were rigged. The decision had already been made.
“Where is she?”
“Bottom of the first hole. About fifty yards down.”
I wriggled through the entrance and scrambled over boulders until the floor disappeared. A vertical drop opened in front of my boots.
“Hi Doc. Just rappel down,” said my team member, his voice drifting up from the dark.
I had rappelled before. Just not inside a cave.
I clipped in and descended through absolute darkness broken only by light from my headlamp. The drop felt like five hundred feet but was probably closer to one hundred; that distinction didn’t matter. It was still a long way up if anything went wrong.
At the bottom, the patient lay wedged between boulders on a small patch of level ground. She was pale, helmeted, and alert.
“House call,” I said.
“Thanks,” she replied. “I’m hurting.”
An EMT gave me a report, but experience had taught me never to outsource the exam in austere environments. By headlamp, I worked through a full assessment—neck and back pain, but no loss of consciousness, no focal neurologic deficit, stable vitals, lungs and abdomen unremarkable. Her mental status was clear.
Nothing declared itself as immediately life-threatening. That did not mean her extrication could wait. In caves, time does not behave.
Our response had been fast for a reason. Someone in her party was a communications engineer. The moment she fell, he exited the cave and improvised a radio link into Tucson’s phone system. She hit the rocks at the same moment the Arizona game hit the final buzzer. Minutes later, our team was activated and moving.
Now came the hard part.
The Neil Robertson stretcher arrived—narrow metal frame, wooden slats, heavy canvas. A device designed for use in mines and transferring patients between ships, not for comfort. I knew it well, having been a patient for one of our cave trainings. The six hours I spent wrapped in that same canvas cocoon while being threaded through a cave had produced a lasting memory. What had been a fifteen-minute walk in became an all-day exit measured in inches. Every stone under the litter transmitted its opinion directly to my spine.
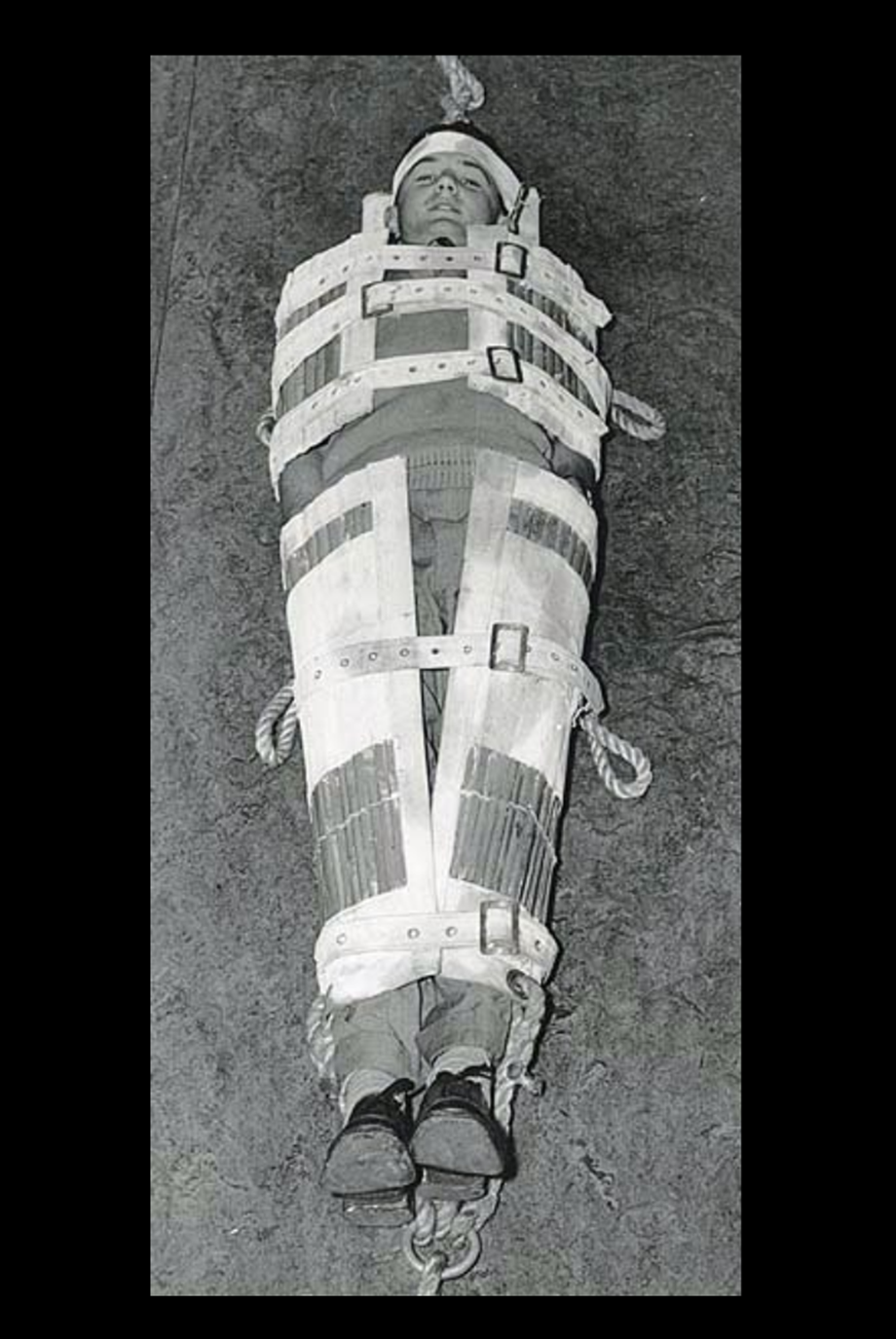
Neil Robertson stretcher. Used via Creative Commons. Photographic Collection from Australia. CC BY 2.0, via Wikimedia Commons.

The author as a simulated cave rescue patient during training with the Southern Arizona Rescue Association. (Photo by Scott Clemens)
That experience had been deliberate. Our rescue association believes you cannot understand cave rescue medicine unless you have occupied both roles. You cannot fully appreciate pain control, IV maintenance, or patient psychology in caves unless you have been immobilized in darkness, tilted and hauled through spaces that appear too small for the stretcher carrying you.
Now, preparing to package this patient, I knew exactly what she was facing.
I told her. She did not appear reassured.
Padding went in. A cervical collar. The integrated helmet and face shield. Straps were tightened in practiced sequence until she was immobilized completely, her world reduced to a narrow field of light and the faces closest to her.
“Any allergies?” I asked.
“No.”
“How do you feel about pain medicine?”
She blinked. “You really brought pain medicine in here?”
“Of course. No house call is complete without it.”
Starting an IV in a cave is an exercise in humility. Cold causes vasoconstriction. Space is limited. Sterility is aspirational. Headlamps flatten depth perception. But the line went in, and the low-dose butorphanol did what good medicine should do—it made a miserable situation more tolerable.
“Much better,” she said.
Two and a half hours after greeting the patient, we began moving her out.
The team kept the stretcher rigorously level as we negotiated the vertical section. A descent that had taken her less than two minutes (including her fall) became a thirty-minute extraction. Rope systems controlled gravity, but only precision controlled safety. Every command mattered. Every hand placement mattered. Trust became physiological. The rope, the harness, the calm voices from below and then above saying, “We’ve got you.”
At the surface, a Huey helicopter waited to carry her the final, most comfortable leg of the journey. Her injuries, although serious, were not catastrophic. She healed.
My own exit came later, via rope ladder. Compared to being in the stretcher, it felt almost civilized.
Climbing back into starlight, I thought of the saying we use in search and rescue: This work will take you places you have never been before and never want to go again.
It is smug. And true. And incomplete.
Because the other truth is this: we keep going back. For the victims—and for our teammates. To be the steady voices in the dark, because we know that the mountains around us are riddled with caves—and yet, with practiced irony, we insist there are no caves to speak of.
Field Competence
This cave rescue, which unfolded over several tense hours on April 2, 2001, occurred early in my involvement with search and rescue—at a point when my medical training far outpaced my understanding of the environments in which it might be applied. It has stayed with me across a quarter century because it exposed, with uncomfortable clarity, how fragile the line is between routine adventure and true catastrophe, and how much hinges on the decisions we make in dark, confined spaces where theory offers no protection. The lesson remains urgently relevant today as more clinicians are asked to provide medical direction for search and rescue teams: familiarity with protocols is not enough. Credibility and safety depend on the ability to function in the field—to move, wait, suffer discomfort, and make decisions within the same physical constraints as the team. Clinicians directing SAR groups must possess not only clinical expertise but also embodied competence matched to the realities of the terrain, standing shoulder to shoulder with rescuers rather than advising only from the safety of distance.
Key Lessons from Cave Rescue Medicine
- Time is unreliable underground. Distances that seem trivial on the surface expand dramatically during extraction. Treatment timelines must assume prolonged transport and delayed reassessment.
- Experience the equipment. Serving as a simulated patient during training reveals pain points, communication barriers, and psychological stressors that directly improve real-world care.
- Spinal precautions should err toward being conservative. As per current guidelines, spinal motion restriction over immobilization is generally optimal; though use of backboards and splints may be necessary for evacuation. (WMS 2024 Clinical Practice Guidelines for Spinal Cord Protection; additional reading on recent updates for spinal cord protection)
- Pain control is not optional. Rigid litters and uneven terrain amplify discomfort. Adequate analgesia improves patient cooperation, reduces physiologic stress, and supports safe extrication.
- Communications save time—and lives. Improvised or preplanned underground communication can dramatically shorten response time. Cultivate relationships with technical and communications specialists.
- Team trust matters as much as technique. Patients placed in total darkness and immobilization rely completely on the competence and calm of the team. Clear communication and steady reassurance are essential clinical tools.