The Chicago Marathon, one of the seven Marathon Majors, is a premier event showcasing both professional and amateur runners (>53,000 runners held in October every year). The race starts at Grant Park, goes through the loop, Lincoln Park, the lakefront, and then the south side and back to Grant Park. I will describe the medical facilities present and injuries encountered during marathons.
The Medical Facilities
The medical facilities included medical tents and a podiatry tent. The main facility was the Balbo medical tent at the finish line, the Jackson medical tent was on Jackson Street, midway in the course was the Laflin medical tent and supply hub, and the Indiana medical tent was the last tent before the finish line. Interspaced over the marathon course were other course medical/aid stations spaced every 1.5 miles (Figure 1).
Each tent had volunteer physicians, physician assistants, and therapists. There was also a staff of psychologists who were present in the main tent. In total, there were about 2,000 volunteers. As the volunteer Attending Physician for the urgent care team, I supervised and oversaw all medical care that was provided including supervision of nurses and other healthcare providers (Figure 2). The goal was to provide medical care based on best practices to participants, spectators, and volunteers as needed. The urgent care had items such as salt tablets, rehydration fluids, band-aids, splints, crutches, and Tylenol (acetaminophen). We had paper medical records in which we documented our history and physical and also our plan and disposition for the patients.

Figure 1: The Chicago Marathon - yellow and red crosses denote medical tent (choosechicago.com)

Figure 2: The Urgent Care Team (Photo credit: Ahmed Nadeem)
There was also a medical observation area (Figure 3) and Intensive Care Unit (ICU) (Figure 4). Runners would come through the finish line and walk to the tent or be brought to the tent on a wheelchair with EMTs who were present throughout the course and would bring injured runners to the closest medical tent. There was a triage team that met the patients upon arrival and then took them to the urgent care team who took care of all types of patients including stabilizing sick ones and transferring them to the observation area or the ICU if they were not getting better in 20 minutes.

Figure 3: The observation floor (Photo credit: Ahmed Nadeem)

Figure 4: The intensive care unit (Photo credit: Ahmed Nadeem)
Musculoskeletal Injuries
Figures 5 and 6 show commonly encountered musculoskeletal injuries in runners. The top five pathologies are usually patellofemoral pain syndrome (17%), shin splints (15%), achilles tendinopathy (10%), plantar fasciitis (4.5%) and iliotibial band syndrome (9%).
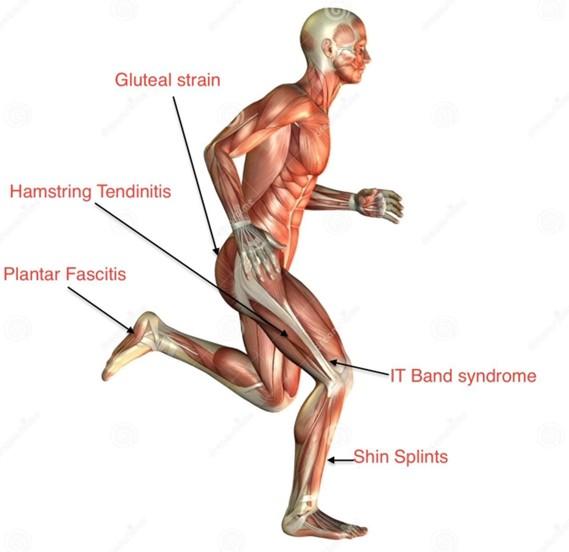
Figure 5: Musculoskeletal injuries in runners
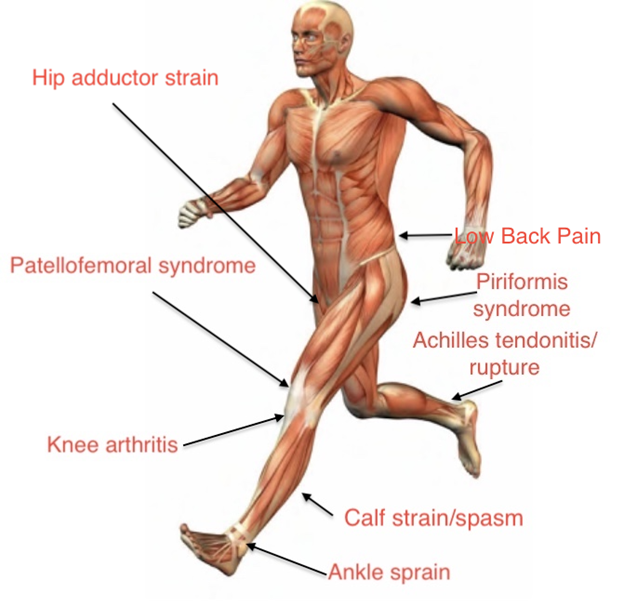
Figure 6: Musculoskeletal injuries in runners
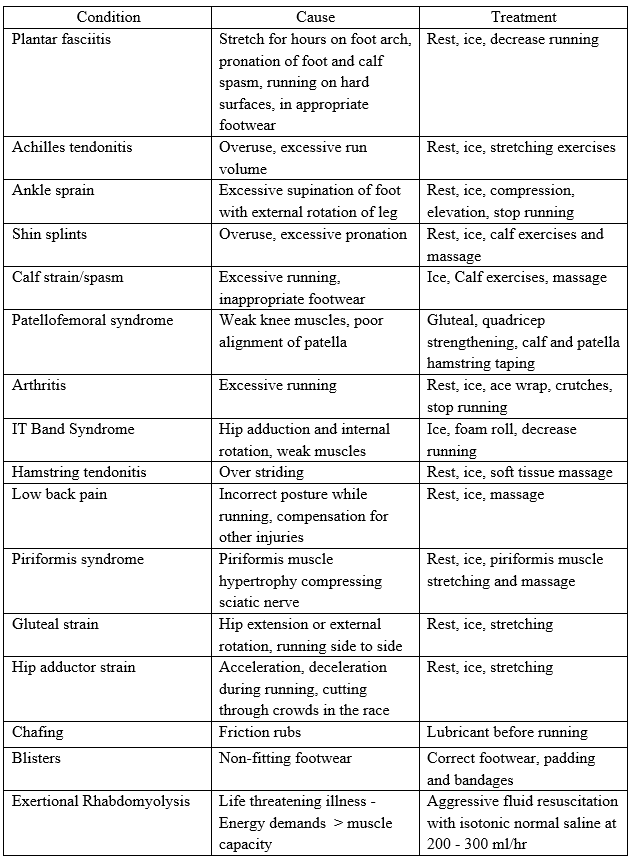
Musculoskeletal Injuries
The table below illustrates the common musculoskeletal injuries encountered during the marathon and their treatment.
Medical Problems
The table below illustrates the common medical problems encountered during the marathon and their treatment.
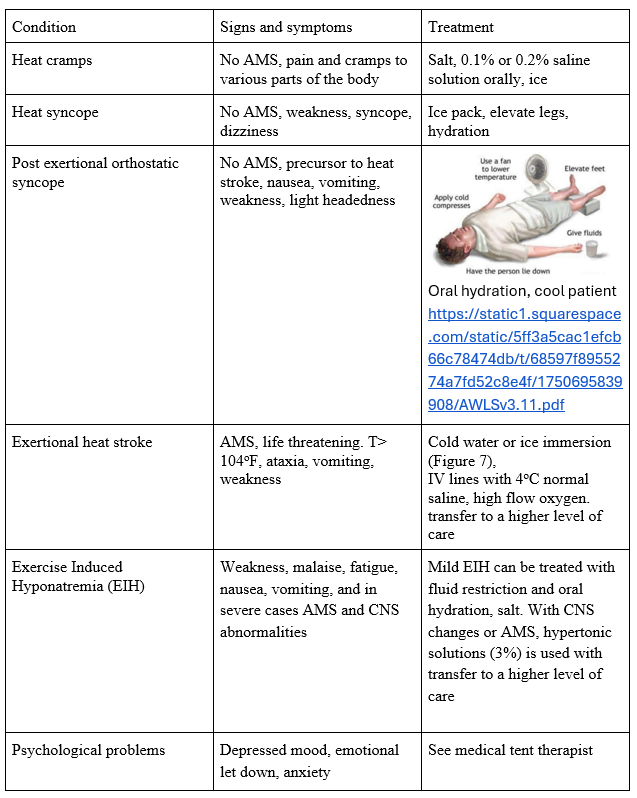

Figure 7: Cold water immersion with ice packs (Photo credit: Ahmed Nadeem)
The Runners
As the race progressed, the number of sick patients increased. Interestingly, the race started with a condition color code of Yellow (Moderate Risk - less than ideal conditions often due to increased temperature or humidity) then Green (Low Risk - good to ideal conditions) during the race. Some runners presented with straightforward problems or a combination of problems such as musculoskeletal pain and heat exhaustion, or might have had an episode of syncope at the finish line. The collapse algorithm (Figure 8) was followed if an athlete was near syncope or unresponsive. It can be seen how important it was to determine the mental status of the patients and that dictated the protocol to be followed. In my tent, we had three runners who had syncope in the tent while being treated for heat exhaustion. Two did well with rehydration, cooling maneuvers, and supportive care. The third ended up having severe hyponatremia and had to be transferred to a higher level of care. We had patients who presented for heat illnesses but did not get better and ended up being transferred to the ICU. We had musculoskeletal injury patients who would not get better at the urgent care and needed to be transferred to the medical observation area. We had no cardiac arrest patients.
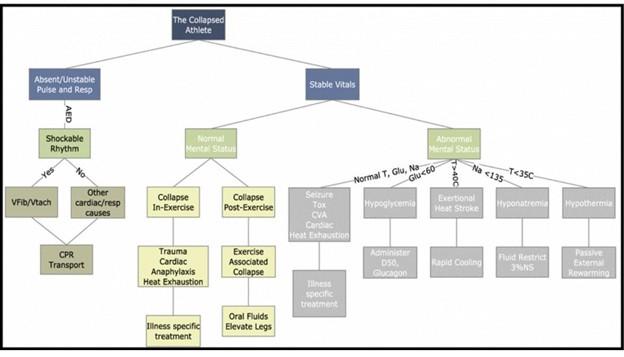
Figure 8: The Collapsed Athlete (Innovative Operations Measures and Nutritional Support for Mass Endurance Events)
Conclusion
I was humbled by the effort the Chicago Event Management took to design all the teams and medical facilities while coordinating with community resources such as the Superior Ambulance Service, Department EMS, and Chicago Police Department. We were well prepared for any scenario including any mass casualty event. Every runner was gracious for the care they received. I look forward to serving there next year.