Introduction
The Wilderness Medical Society (WMS) convened an expert panel to review and update clinical practice guidelines for the prevention and management of burn injuries in austere environments. The 2025 update emphasizes evidence-based recommendations relevant to resource-limited settings, prehospital environments, and wilderness contexts. This summary outlines key recommendations for burn classification, initial assessment, wound care, fluid resuscitation, analgesia, infection prevention, and evacuation considerations.
Initial Burn Assessment
Initial priorities include ensuring scene safety and addressing life-threatening conditions. Management should follow standard trauma protocols using the ABCDE approach. Begin by assessing the airway, breathing, and circulation. Inhalation injury should be suspected if the patient has facial burns, singed nasal hairs, soot in the oropharynx, hoarseness, or soot-tinged sputum. Patients with suspected inhalation injury require early oxygen supplementation and prompt evacuation. Patients with indications for airway management in the field should be intubated if appropriate medications and equipment are available, including sedation and paralytics.
Evaluate for associated trauma, particularly with electrical or blast injuries. Hypothermia should be prevented during the evaluation and treatment process.
Burn Classification
Burn depth is categorized into superficial, partial-thickness (superficial and deep), and full-thickness injuries. Superficial burns affect only the epidermis, presenting as red, painful, and dry without blistering. Partial-thickness burns involve the dermis and are subdivided: superficial partial-thickness burns are moist, red, and blistered, while deep partial-thickness burns appear pale, mottled, and may be less painful due to nerve damage. Full-thickness burns extend through the dermis, appear dry and leathery, and are insensate.
Burn size is estimated using the Rule of Nines for adults or the Lund and Browder chart for children. (Figure 1). Alternatively, the patient’s palm (including fingers) can be used to estimate approximately 1% of total body surface area (TBSA). Accurate TBSA estimation guides fluid resuscitation and disposition.

Burn Cooling and Wound Care
Wound management begins with stopping the burning process and cooling the burn with clean, cool (not cold) water for up to 20 minutes, ideally within 1 hour of injury. Cooling can reduce pain, edema, and tissue damage. However, prolonged cooling or the use of ice should be avoided due to the risk of hypothermia or further tissue injury. After cooling, the wound should be gently cleaned if possible. Remove clothing and jewelry near the burn site, as they may continue to smolder or be at risk of causing constriction injury due to expanding tissue from swelling.
Cover burns with a clean, dry dressing. Non-adherent gauze is preferred. Burned hands and feet should have dressings placed between digits to prevent adherence. Bulky dressings may be needed to reduce pain and protect the wound.
Topical antimicrobials may not be available in austere settings. If available, antibiotic ointment or honey may be applied on deep partial-thickness burns if attempting field management or if evacuation will be delayed. If available, absorbent foam dressings such as Mepilex may be used on superficial partial-thickness burns and left in place for a week to avoid serial dressing changes. If evacuation is expected in less than 12-24 hours, clean, dry dressings without the use of ointments will suffice.
Blisters should generally be left intact. If a blister is large, tense, or likely to rupture during evacuation, clean needle aspiration may be considered in some cases. Do not debride blisters in the field due to a poor sterile environment and access to adequate analgesia.
Pain Management
Burn injuries cause significant pain and require early and ongoing analgesia, particularly during wound care or evacuation. Non-opioid analgesics (e.g., ibuprofen, acetaminophen) should be administered if not contraindicated. Opioids and/or ketamine may be needed for moderate to severe pain but may not be available in all austere environments. Pain control should be tailored to the severity of the injury and available resources.
Pain management should be titrated to patient comfort while minimizing side effects. Non-pharmacologic techniques, including splinting and minimizing dressing changes, may also be beneficial.
Fluid Resuscitation
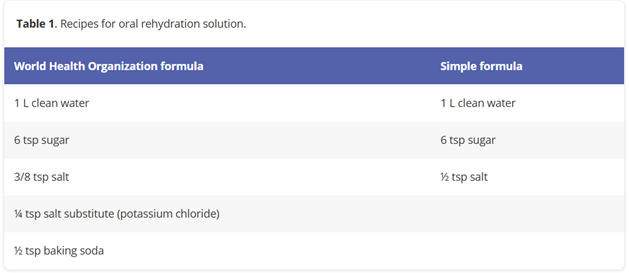
Patients with burns involving more than 20% TBSA (partial or full thickness burns) generally require fluid resuscitation. In remote settings, begin oral rehydration if the patient is alert, not vomiting, and has a functional gastrointestinal tract. Use electrolyte-containing solutions if available. Oral fluid resuscitation has been used for burns up to 40% TBSA in low-resource settings. Oral rehydration solution may be improvised if no commercial products are available. (Table 1).
For patients who cannot tolerate oral fluids or are more severely burned, initiate intravenous fluid resuscitation. The Modified Parkland formula (2 mL/kg per % TBSA burned) using lactated Ringer’s solution is recommended, with half administered in the first 8 hours post-injury and the remainder over the following 16 hours. Adjust based on urine output and clinical status. In the absence of lactated Ringer’s, normal saline is acceptable.
Frequent reassessment is essential, and signs of under- or over-resuscitation should be monitored. Urine output, while ideal, may be impractical to monitor in the field. Capillary refill, mental status, and peripheral pulses can help guide fluid therapy in resource-limited settings.
Infection Prevention
Burn wounds are highly susceptible to infection. However, prophylactic systemic antibiotics are not recommended in the prehospital or austere environment, as they do not prevent wound infection or sepsis and may contribute to antimicrobial resistance. Treatment should focus on proper wound care and cleanliness to minimize infection risk. Systemic antibiotics may be considered if there is clear evidence of systemic infection (e.g., fever, increasing erythema, purulence, or signs of sepsis), based on provider judgment and resource constraints.
Special Considerations
Electrical burns may cause deep tissue injury not evident on initial inspection and increase the risk of compartment syndrome or cardiac arrhythmias. Monitor for signs of rhabdomyolysis (e.g., dark urine), and maintain high urine output if suspected.
Chemical burns require immediate removal of contaminated clothing and copious irrigation with water. Specific antidotes are rarely available in austere settings. Avoid attempting to neutralize chemicals with other chemicals.
Circumferential full-thickness burns may impair circulation. Monitor distal pulses and capillary refill. Escharotomy may be needed in rare cases but should only be performed by trained providers.
Evacuation and Disposition
Evacuation decisions should be based on burn severity, resource availability, and the patient's clinical condition.
Burns requiring evacuation include:
- Burns >10% TBSA in adults
- Burns of critical areas (face, hands, feet, perineum, or major joints)
- Full-thickness burns
- Electrical or chemical burns
- Inhalation injuries
- Burns with suspicion of carbon monoxide or cyanide toxicity
- Burns that require extensive debridement, escharotomy, or fasciotomy
- Burns in patients with comorbidities, associated trauma, or hypothermia
Evacuation should be prioritized for patients with airway compromise, extensive burns, or signs of systemic illness. Protect wounds with clean dressings and maintain hydration and pain control during transport.
Conclusion
The 2025 Wilderness Medical Society update on burn care provides clinicians and first responders with evidence-based guidelines tailored for austere environments. Emphasis is placed on early assessment, appropriate wound care, pain control, hydration, and timely evacuation when needed. These recommendations are intended to improve outcomes for burn-injured patients in wilderness, prehospital, and remote settings.