Introduction
When people think of the causes of climate change, they probably don’t think of their doctor’s office or their local hospital, but the reality is that the health care industry is responsible for nearly 10% of all greenhouse gas emissions in the United States (US). Pharmaceuticals are responsible for 20% of those healthcare emissions; not all drugs are equally responsible, with anesthetic gases and metered dose inhalers accounting for 1% of all healthcare emissions. Pharmaceuticals have a significant impact on our contribution to climate change as clinicians, and we can choose medications that have lower impacts without compromising patient care and often reduce the cost of care.
Metered Dose Inhalers
Metered dose inhalers (MDIs) have used a hydrofluorocarbon (HFC) propellant to deliver medication to the patients’ lungs since the 1990s. HFCs replaced an older propellent, chlorofluorocarbons (CDCs), which were ozone depleting chemicals. While this switch was an improvement, HFCs are still potent greenhouse gases with a single dose (two actuations or “puffs”) releasing the equivalent of 164 to 238 grams of CO2. A single MDI produces as much CO2 emissions as driving a standard gas-powered car 175 miles. Dry powdered inhalers (DPIs), alternatively, use the patient’s own inhalation to deliver the medication and by eliminating the HFC propellant, have a significantly lower carbon footprint, equal to just 4 miles of driving a car per use. Not all patients are able to use DPIs, including very young patients or those with severe restrictive lung disease, but in the US, nearly 80% of inhalers are prescribed in the MDI form, essentially 550,000 cars worth of emissions, when countries like Sweden prescribe more than 80% of inhalers in the DPI form, with similar or better patient- centered outcomes. In 2020-2021, the carbon emissions from MDIs in the National Health System in Scotland were larger than emissions from fleet vehicles.
Figure 1: Infographic showing use an MDI being equivalent to driving a gas powered vehicle 175 miles (the distance from London to Sheffield) versus the use of a DPI being equivalent to driving 4 miles. Source: NHS Suffolk and North East Essex
CASCADES, a Canadian Climate Action and Health initiative, outlines a five step plan for climate-conscious inhaler prescribing. Key recommendations include: confirming the diagnosis, controlling the disease, considering inhaler type, optimizing technique, and proper disposal. The UK’s National Institute for Health and Care Excellence (NICE) guidelines for asthma treatment recognize the importance of choosing environmentally sustainable treatment options when possible. In combating inhaler impact on the environment, it is important to address improper diagnosis and lack of disease control as both lead to overprescribing, increased use of unnecessary inhalers, and, ultimately, increased greenhouse gas emissions. Improper inhaler technique is also a key component as it may lead to poor disease control, increased prescribing, and use of multiple inhalers.
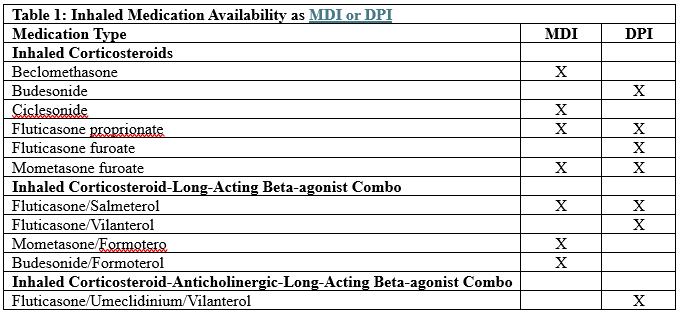
In 2022, a study showed that switching from an MDI to a DPI reduced the carbon footprint of the total treatment (rescue and maintenance therapy) by half and showed a 10-fold reduction when looking at maintenance therapy alone, all while maintaining disease control, showing that efficacy is not lost in pursuing this change. A study out of Ottawa, Canada showed that 90% of MDI doses dispensed in a hospital were unused, leading to a great deal of waste with environmental impacts. This is especially important as the canister, even when considered empty, still has propellent in it and about 30% of greenhouse gas emissions from inhalers occur upon disposal due to propellant leakage. Proper disposal through recycling programs, drug-take-back days, or prepaid mailers for inhaler return provided by some pharmacies is important. Availability of options may vary by country and region. Utilizing one of these disposal programs ensures the remaining propellent is destroyed correctly by hazardous waste management facilities that can do so in an environmentally friendly manner. Table 1 lists drugs available as an MDI or DPI.
Nitrous Oxide and Other Anesthetic Gases
Since the mid-1800s nitrous oxide (N2O), also known as “nitrous” or “laughing gas”, has been used as an inhaled anesthetic. Many hospitals have large tanks of N2O housed in a basement, connecting to operating rooms and labor and delivery suites through pipes that span throughout the facility walls. These piping systems are prone to leaks and many studies have shown that the majority of nitrous purchased never reaches the patient, with one study showing that up to 99% of the N2O purchased was unaccounted for due to off-gassing into the atmosphere through these leaks. Not only is this a financial waste, but it also creates a large impact on the environment. N2O’s impact on global warming is nearly 300 times that of carbon dioxide, leads to greater destruction of the ozone layer than chlorofluorocarbons, and remains in the atmosphere for over 100 years.
Healthcare systems around the world have begun to decommission central supply of N20, discontinue purchasing large amounts, and have moved to utilizing small, portable canisters instead when needed. The University of California San Francisco (UCSF) projects an 80% decrease in contribution to off-gassed N2O, which is comparable to a reduction in 2.7 million fewer miles driven, with these changes. Another healthcare facility found switching from centrally supplied to portable canisters reduced emissions from 594 mtCO2e per year to 5.6 mtCO2e per year. A group of healthcare leaders within the Pacific Northwest, known as Cascadia Collaborative, have developed a playbook for “discontinuing use of piped nitrous oxide systems in healthcare facilities”. This playbook walks clinicians through assessing opportunities, engaging stakeholders, communicating the value, and transitioning to a portable N20 cylinder supply.
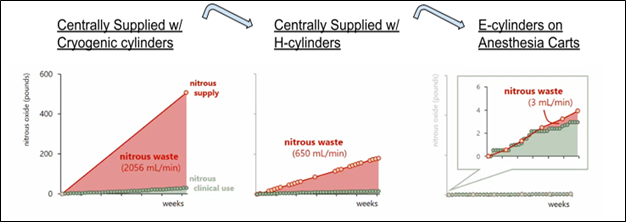
Figure 2: Diagram showing how one facility’s N2O losses due to leakage (red) compared to their clinical use (green) as they changed from central supply to portable cylinders. Source: Cascadia Collaborative
The World Federation of Societies of Anesthesiologists provides a statement supporting environmentally friendly anesthetic practice promoting, in a tiered approach, halothane followed by sevoflurane use over isoflurane and note that desflurane and N2O should be reserved for specific cases. Additionally, more than half of this group believes regional anesthesia is preferred followed next by intravenous anesthesia, and inhaled anesthetic gases should be used last, specifically calling out environmental concerns with use of anesthetic gases. Desflurane, a highly potent inhaled anesthetic with a global warming potential 3,700 times that of carbon dioxide, remains widely used, but alternatives including sevoflurane or isoflurane, have similar clinical efficacies, lower global warming potentials and a lower cost.
There is no standard for hospitals to capture or reduce waste these gases create during surgical procedures. When given to a patient, only a small amount is utilized to achieve sedation while up to 95% is exhaled by the patient as waste. Exhaust systems exist to remove the exhaled waste and prevent hospital staff from becoming impaired. These exhaust systems, however, typically vent this waste to the environment outside, contributing to greenhouse gas emissions. One study found the environmental impact of desflurane during one surgery had the same impact as driving 12 diesel powered Humvees for the same time frame as the procedure.
Like decommissioning central supplied N2O, efforts to reduce the impact of inhaled desflurane and other anesthetic gases is catching traction too. Facilities can work to ensure their anesthesia machines are newer, more efficient models with advanced carbon dioxide absorbers and lower flow rates. Additional efforts include working with pharmacy and anesthesia stakeholders to reduce purchase and use of desflurane and N2O, specifically.
In addition to reducing environmental impact, there is cost reduction to avoiding these gases as well. In 2020, St. Luke’s Health System in Idaho implemented an initiative to reduce their environmental impact by encouraging sevoflurane utilization over desflurane. Through physician education and policy change, desflurane use decreased substantially. This change in practice saved over 1,000 metric tons of CO2e in a two-year period which equates to 2,745,498 miles driven by an average gasoline-powered passenger vehicle or 110 laps around the world. Additionally, they were able to show a cost saving of $242,000 in the same time frame. Harborview Medical Center in Seattle showed a reduction in spending of 27% through utilization of more efficient models of anesthesia machines and another study showed a cost savings of almost $200,000 per year by implementing an initiative to reduce desflurane use by 50%. Many other institutions, too, have worked to reduce desflurane use while reaping the benefits of cost savings this practice change brings. In 2022, the American Society of Regional Anesthesia and Pain Medicine published a newsletter supporting this practice change as a way to “green” the operating room and specially call out the price difference, environmental impact, and lack of evidence supporting use of desflurane over sevoflurane.
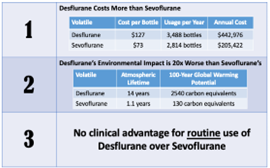
Figure 3: Cost and usage information at one facility for desflurane versus sevoflurane. Source: American Society of Regional Anesthesia and Pain Medicine
Conclusion
Clinicians can begin to make practice changes surrounding pharmaceuticals that have a positive impact on reducing greenhouse gas emissions. Targeting three main pharmaceutical classes - MDIs, N2O, and anesthetic gases - is a good place to start. Clinicians can prescribe DPIs in place of MDIs when appropriate, educate patients on disposal options, and focus on de-prescribing through confirmation of necessity of the inhaler and ensuring proper inhaler technique. Clinicians can also work with their institutions to decommission the use of centrally supplied N2O gas for bedside canisters instead, in places where N2O is still utilized. Lastly, clinicians can work with anesthesia partners to ensure their machines are updated to more efficient models and to develop guidelines for a tiered approach anesthetic medication use supported by World Federation of Societies of Anesthesiologists with utilizing IV medications over gases and using sevoflurane over desflurane when gas is needed. Initial steps such as these can begin today and can lead to other larger system changes to help protect our environment against pharmaceuticals that produce harmful greenhouse gas emissions.