I’ve spent most of my professional life managing risk in the wilderness. For nearly three decades, I worked with outdoor programs where crisis response, though infrequent, was a critical necessity. When there was a significant incident—a severe injury, a missing participant, or in the worst cases, a fatality—our team gathered, activated our crisis plan, and began to respond. Each incident was intense and complex, but we moved steadily through the response phases.
At the heart of this approach was a core assumption: Crises are acute, singular, and resolvable. Then I shifted into the field of climate and health, and that assumption began to unravel.
Traditional wilderness risk management is predicated on the idea that emergencies are temporary. But climate change is replacing “acute” with “ongoing.” It is replacing “singular” with “cascading.” And it is demanding that we develop a new kind of preparedness, one rooted not just in emergent response, but in systems thinking, long-tail recovery, and climate science fluency.
Hurricane Helene made landfall in the southeastern United States in late September 2024, unleashing torrential rain, flooding, landslides, and widespread infrastructure failure. Two hundred and fifty people died in the immediate aftermath but the true toll is yet unknown. A recent Nature study estimates that 80% of excess deaths from Helene will occur between three and fifteen years after the storm, due to the impacts of chronic stress on health, inadequate and inequitable resources for rebuilding, and breakdowns in public support systems. That’s potentially tens of thousands of lives lost not from wind or water, but from systemic fragility and lack of resilience.
Sadly, Helene in not unique.
One of the most critical insights in climate-driven disaster response is that the past is no longer a reliable predictor of the future. Labeling events as “once in a hundred years” no longer reflects reality and causes us to dismiss them as outliers. The new normal is a pattern of compounding, increasingly severe events. In 2024 alone, NOAA identified 27 separate billion-dollar weather and climate disasters with a dangerous upward trend over the past decade.
Just as historical norms no longer define the future, our traditional approach to preparing for climate-amplified disasters falls short. Clinicians, even those whose traditional roles don’t include disaster response, have a crucial role to play in preparation and adaptation.
The University of Colorado’s Diploma in Climate Medicine, an affiliate of the Wilderness Medical Society, is one example of a program trying to build literacy and leadership across the skill set that will be needed for our future. Whether it is climate change communication and advocacy, healthcare system decarbonization, or a detailed understanding of the health impacts of climate change, programs like this help care providers challenge outdated assumptions and build resilience in a fast-changing world.
During the recent Certificate in Disaster Resilience and Response, one of the five Certificates in the Diploma program offered annually, participants were challenged to rethink effective preparedness. They traveled to College Station, TX, home of Texas A&M Engineering Extension Service (TEEX), to immerse themselves in a multi-day simulation based on a real-world event. The complex scenario pushed them to grapple with hard decisions: When should the Incident Command System and crisis standards of care be implemented? What happens when hospitals must close? How do we prepare an exhausted workforce to respond to overlapping emergencies? What is the emotional toll of managing difficult ethical decisions?
To deepen their learning, participants also took part in Disaster Day, a large-scale, interdisciplinary simulation hosted at TEEX’s 52-acre Disaster City. Originally a small training for Texas A&M medical and nursing students, Disaster Day has grown into one of the nation’s most comprehensive preparedness simulations. It now engages pharmacy, public health, dentistry, and professional responders. The University of Colorado cohort joined this 750-person simulation, bringing awareness of the unanticipated complications of climate-fueled disasters. Working alongside seasoned first responders, participants explored real-world challenges in triage, critical care transport, shelter operations, patient evacuation, and incident command systems. Most importantly, they gained firsthand experience with the National Response Framework in action, enhancing their understanding of the interconnected structure utilized during complex emergencies.

Diploma in Climate Medicine participants at Disaster City, in College Station TX (Photo credit: Shana Tarter).
Given that most participants are unlikely to serve as the Incident Commander during a hospital evacuation, why is this training important? Much like our healthcare facilities and associated essential equipment which were built without climate resilience in mind, our emergency operations and patient response plans have typically not been designed with a future-focused lens. The wilderness medicine community is uniquely positioned to lead in this future. We are already experts at adaptability, improvisation, and operating in unpredictable conditions. But in a world of extended power disruptions, prolonged environmental stressors, and novel disease outbreaks, our education must evolve to match the scale and complexity of the threats ahead. Our toolkit must now include climate science fluency, systems thinking, and policy engagement.
Through my work with the Wilderness Climate Action Lab, I’ve taken many of these insights back to the outdoor program community to help organizations build Climate Resilience Plans. Last year we gathered input from 127 outdoor programs to establish baseline data on the impact of climate change on operations. The results of this survey are available in the Climate Change & Health Special Topic Section of the March 2025 Journal of Wilderness & Environmental Medicine. The industry response was clear, the impacts of climate change are already being felt and organizations are struggling to adapt. Nearly 60% of respondents reported having to revise between 4 and 20 program days during the 2023 season. Programs identified large knowledge gaps in identifying trusted sources of information, new legal exposures, and the health and medical implications of short- and long-term exposure to climate change-induced hazards such as wildfire smoke.
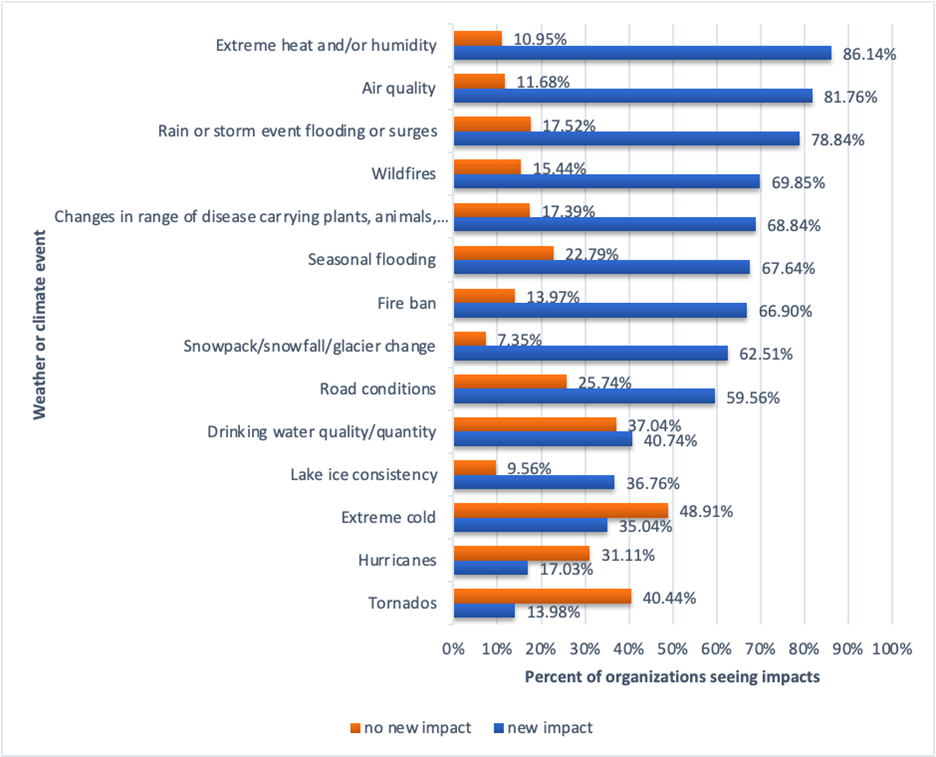
Figure 1: Percent of outdoor organizations seeing impacts from weather or climate events in 2023 compared to previous three years. (Wilderness & Environmental Medicine)
It is clear we must plan differently. For those who venture into the outdoors, we should assume we will be managing severe weather events, wildfires and smoke, and vector-borne diseases in new places. Every trip must have an established alternative. Organized programs must plan to sustain themselves financially through periods of closure and must be extremely skillful at hazard assessment and risk communication with our participants.
Whether you are an outdoor organization or a health care clinic, continuing to operate with a business-as-usual mindset is a sure pathway toward the heightened stress and inefficiency of reacting to disruptions and incidents rather than preparing for them. Now is the time to invest in our resilience and acknowledge that our outdated perception of crisis planning must evolve. It is essential that we plan for the conditions we’ll face 20 years from now - not rely on the realities of 20 years ago.