
Introduction
The Tactical Combat Casualty Care (TCCC) Guidelines, the standard for battlefield trauma care in the US Department of Defense, offer comprehensive best-practice recommendations for combat medical personnel at the point of injury. Before 2024, they recommended nasopharyngeal or supraglottic airway devices before definitive surgical airway management. In January 2024, the Committee on Tactical Combat Casualty Care (CoTCCC) released an update after a multiyear review challenging dogmatic assumptions about airway management in the prehospital environment. They found that most airway technique and equipment reviews are conducted for civilian emergency medical services (EMS), focusing on out-of-hospital cardiac arrest (OHCA). Recognizing this complex comparison, the CoTCCC carefully reviewed civilian literature.
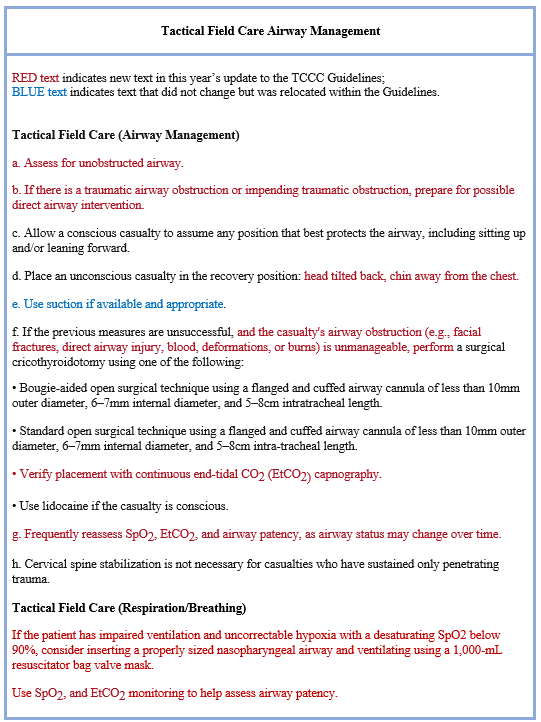
A direct outcome of the CoTCCC review is the simplification of the airway management sequence during Tactical Field Care. Deaton et al. published these changes in March 2024 in the Journal of Special Operations Medicine (Table 1). However, the publication lacked discussion about the rationale and evidence supporting these changes. The updated TCCC airway management and other guidelines are available on the Deployed Medicine website. To access tactical combat casualty care content, you must create an account with a username and password to meet Defense Information Systems Agency cybersecurity requirements.
Table 1. Tactical Combat Casualty Care Airway Management Guidelines Update 2024.
Based on the Deaton et al paper, in April 2024, we published the first of two articles in Wilderness Medicine Magazine entitled “Tactical Airway Management Update (Part 1).” Two significant changes in TCCC airway management for Tactical Field Care were removing supraglottic and nasopharyngeal airways. These changes may surprise readers, especially those in civilian prehospital care, as nasopharyngeal and supraglottic airways have been fundamental recommendations for advanced airway management. This article provides the rationale, recommendation, and level of evidence for the modifications to the airway management guidelines as detailed by Shaw et al. We also discuss pertinent TCCC airway management modifications that may be appropriate for wilderness medicine providers. Finally, we present the TCCC airway management skill applicable to any first responder in an austere environment and discusses basic and advanced airway kits for backcountry travel.
Tactical Combat Casualty Care Airway Changes: 2024
The airway and breathing/respiration update to the TCCC Guidelines were made to the following areas: 1) positioning of the patient, 2) nasopharyngeal airways, 3) supraglottic airways, 4) tracheal intubation, and 5) surgical cricothyroidotomy. A summary of the TCCC airway, and breathing/respiration changes is listed below.
TCCC Airway Management in Tactical Field Care
- Simplifies the airway management sequence in Tactical Field Care (TFC).
- Better defines the recovery position with the head tilted back and chin away from the chest.
- Eliminates extraglottic airways.
- Removes nasopharyngeal airways from TFC and adds to Respiration / Breathing section.
- Provides more specific indications for surgical cricothyroidotomy.
- Establishes the need for frequent reassessment of SpO2, EtCO2, and airway patency.
TCCC Respiration / Breathing in Tactical Field Care
See Table 2 for some of the key TCCC airway changes along with the rationale of change, CoTCCC recommendations, and level of evidence, which is based on the CoTCCC paper published in the Journal of Special Operations Medicine in December 2024 – see Shaw et al for a thorough presentation of these topics.


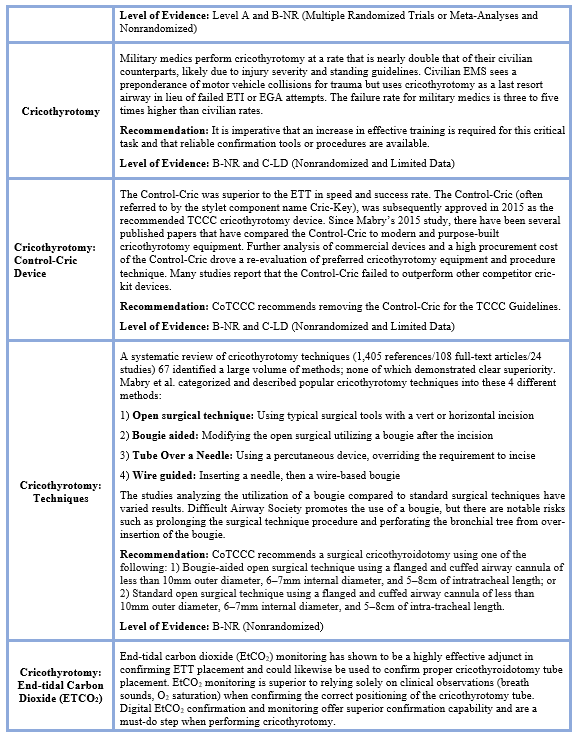

*The Committee on TCCC and TCCC Guidelines utilize the ACC/AHA (American College of Cardiology/American Heart Association) evidence classification system to ensure that recommendations are based on the highest quality of evidence available, adapted to the unique challenges of combat medicine.
Level A - High-quality evidence for more than one randomized control trial (RCT); Meta-analyses of high-quality RCT; one or more RCTs corroborated by high-quality registry studies.
Level B-NR (Nonrandomized) Moderate-quality evidence from 1 or more well-designed, well-executed nonrandomized studies, observational studies, or registry studies; Meta-analyses of such studies.
Level C-LD (Limited Data) Randomized or nonrandomized observational or registry studies with limitations of design or execution; Meta-analyses of such studies.
Implications for the Wilderness Medicine Provider
Previous publications by Bennett et al. and Butler et al. have demonstrated the applicability of the TCCC Guidelines for wilderness medicine providers who encounter airway and respiration management challenges. Given that the TCCC Guideline now predominantly focuses on body positioning, suction, and surgical cricothyroidotomy, the question arises as to how best to integrate these newly updated airway management guidelines by wilderness providers. The answer is not binary, yes-or-no decision; rather, it involves determining when, where, and why to apply these updated guidelines. Whether in a battlefield setting or a backcountry environment, there are situations where the use of nasal or oral airways may not be practical or effective for managing the airway. The reader is also referred to the CoTCCC airway management training guide.
In any limited resource environment with or without an airway kit, the goal for basic airway management, whether there is blunt or penetrating trauma to the neck or face, still can be achieved without definitive resources, such as video laryngoscope for tracheal intubation, power suction, and high-flow oxygen. The most critical goal is to ensure the patient can breathe effectively so that oxygen can be delivered to the lungs. For example, whether you’re on the battlefield or in a wilderness setting this is achieved by manually opening and clearing the airway along with ongoing vigilance to maintain an open airway.
As outlined in two case reports (1) and (2), which describe patient falls from height and a different approach for airway management based on location, resources, and manpower. A conscious patient should be permitted to assume a comfortable position. For an unconscious patient, they are positioned in a lateral recumbent position with the head tilted back, allowing the chin to be positioned away from the chest. These two positions are fundamental interventions for either the first responder or advanced care practitioner. This position utilizes gravity to safeguard the airway from common obstructions such as saliva, viscous secretions, blood, and vomit. To enhance the lateral recumbent position, we recommend retaining oropharyngeal airways, nasopharyngeal airways, and extraglotic airways based on your frequency of use and annual refresher training. It is essential to be familiar with the limitations as outlined above by the CoTCCC for airway devices including proper sizing, use with facial and airway trauma, use in extreme heat and cold temperatures, and in altitude during aeromedical evacuation.
Strongly consider adding a small commercial or improvised suction device. Two examples of commercial suction devices available are by North American Rescue and EverGuard, which are small, lightweight, one-handed, and reasonably priced for a backcountry airway kit. Alternatively, an improvised suction device can be constructed by inserting a large syringe (typically 60 mL) into the lumen of a 30FR (French) nasal airway trumpet. This creates a portable suction device. However, this improvised device may have limitations compared to commercial devices mentioned above, as it cannot effectively clear substantial amounts of emesis from the airway when the head position is not in a gravity-assisted manner. Additionally, it requires practice with two hands to operate effectively.
In an advanced airway kit for backcountry use, add a 1000-mL adult, or 500-mL pediatric BVM for adequate ventilation, which is less likely to cause pulmonary barotrauma. Carry a small commercial tracheal intubation kit and a small commercial cricothyrotomy kit, commonly used in tactical medicine. Follow and train with cricothyrotomy equipment and techniques as outlined by Shaw et al. Carry medications for pain control and rapid sequence induction (RSI). Without pre-hospital RSI for deep sedation or muscle relaxants, insertion of EGAs and tracheal intubation is only tolerated in deep comatose patients.
Final Thoughts
Airway management, regardless of the location (front country or backcountry), can be particularly challenging, especially when the familiarity of equipment and techniques carried in a medical kit is not frequently practiced. The TCCC Guidelines for airway management can be applied to wilderness providers with the knowledge of their limitations in specific scenarios when nasal and oral airway devices are considered. Which airway equipment is carried in your airway kit is your preference, as long as the principles of basic and advanced airway management are adhered to. Note: The authors have no affiliation with any commercial product listed in this article.