Epinephrine, also known as adrenaline, is an endogenous hormone and neurotransmitter, also available as a medication. Produced by the adrenal glands, epinephrine (and norepinephrine) are responsible for the “fight or flight” response during stressful situations. When administered as a drug, epinephrine produces the same clinical effects as the endogenous hormone on the lungs, heart, and skeletal and vascular smooth muscles by stimulating alpha- and beta-adrenergic receptors. In the lungs, epinephrine causes bronchodilation, in the heart, increased cardiac contractility and heart rate, and in skeletal and vascular smooth muscles, vasoconstriction leading to increased blood pressure and mean arterial pressure.
The FDA has approved epinephrine for several indications including anaphylaxis and other severe immediate hypersensitivity reactions, hypotension or shock, and mydriasis during intraocular surgery. In addition to the labeled indications, off-label indications are abundant, such as acute and severe asthma, atrioventricular block in symptomatic or hemodynamically unstable patients, symptomatic or hemodynamically unstable (unresponsive to atropine) bradycardia, cardiogenic shock, inotropic support, post-cardiac arrest shock, and sudden cardiac arrest due to asystole, pulseless electrical activity, ventricular fibrillation, or pulseless ventricular tachycardia. Depending on the indication, epinephrine can be administered by various routes – intravenous, intramuscular, subcutaneous, endotracheal, intraosseous, inhalation, ophthalmic, and now, intranasal. The drug cannot be taken orally as it is metabolized too quickly in the GI tract to achieve therapeutic levels, and cannot be administered by metered-dose inhaler as it is too difficult to take multiple puffs quickly enough to achieve sufficient blood concentrations for anaphylaxis.
In wilderness medicine, epinephrine’s most common use is for anaphylaxis and other severe immediate hypersensitivities. Anaphylaxis is a type I IgE-dependent immediate hypersensitivity reaction that affects multiple organ systems. The diagnosis of anaphylaxis is determined by the sudden onset of symptoms within minutes to hours after exposure to a trigger. Individuals may meet the clinical criteria for anaphylaxis in three ways, as seen in Figure 1 below.

Figure 1. Guidelines for the Assessment and Management of Anaphylaxis (WAO)
Cutaneous and mucosal involvement is the most frequent sign of anaphylaxis (in 80-90% of patients). The clinical symptoms for this presentation include urticaria (hives), flushing, pruritus (itching), oropharyngeal swelling or angioedema causing difficulty breathing or wheezing, or low blood pressure. Other organ involvement includes: respiratory tract (lower airways; up to 70%), GI tract (up to 45%), cardiovascular system (up to 45%), and central nervous system (up to 15%).
Epinephrine is the first-line treatment for anaphylaxis; it prevents and relieves airway obstruction due to mucosal edema and causes vasoconstriction in the vasculature to prevent hypotension. The dosage is: Adults and children >30 kg (66 lbs): 0.3 to 0.5 mg intramuscularly or subcutaneously into the anterolateral aspect of the thigh every 5 to 10 minutes as necessary; children <30 kg (66 lbs): 0.01 mg/kg up to 0.3 mg. In a wilderness setting, the most common administration route is intramuscularly via auto-injector (generic forms of EpiPen and Adrenaclick are now available for ~$200-300 for 2 pens; Figure 2) or IM using a multidose vial (1mg/mL; up to 2 doses) and syringe (Figure 3), which is far cheaper than the auto-injector, but requires training to administer.

Figure 2. Generic epinephrine auto-injector.

Figure 3. Epinephrine multidose vial. Photo by Nancy Pietroski.
Randomized controlled trials have shown that the intramuscular injection of epinephrine into the thigh leads to peak plasma concentrations in the shortest period. Injections into the subcutaneous space or the deltoid muscle lead to decreased plasma concentrations and erratic absorption in the body – therefore these routes should be avoided (even though the prescribing information for the auto-injector states subcutaneous as an acceptable route).
In August of 2024, the FDA approved Neffy® 2 mg epinephrine nasal spray, a needle-free epinephrine product, for the treatment of type I allergic reactions including anaphylaxis in adults and children who weigh at least 30 kg (66 lbs). In March of 2025, Neffy® 1mg was approved for patients who are 4 years old and weigh at least 15 kg (33 lbs). Identical to other epinephrine products, Neffy® acts on alpha- and beta-adrenergic receptors in the body. The product is available by prescription only.

Figure 4. Neffy® nasal spray.
Neffy® 2 mg/0.1mL nasal solution is sprayed once into one nostril in adult patients or pediatric patients who weigh > 30 kg. For pediatric patients ≥ 4 years old who weigh ≥15 kg to < 30 kg, Neffy® is administered as one spray in one nostril using a 1 mg/0.1mL nasal solution. If symptoms persist, a second dose should be administered in 5 minutes in the same nostril. Each spray is for single use only and delivers the full dose upon activation. Unlike other nasal sprays, users should not prime or attempt to reuse Neffy®.
To administer Neffy®, insert the nozzle of the nasal spray into one nostril until the fingers can touch the nose. Users should hold the nasal spray straight, pressing the plunger firmly to deliver the dose. Do not angle the nozzle, as some medication may be lost during administration. If a second dose is necessary, a new nasal spray should be inserted into the same nostril 5 minutes after administration of the last dose. The package insert instructs users to use the right hand to administer Neffy® to the right nostril and the left hand to administer to the left nostril to ensure proper drug administration. Patients should seek medical advice following the use of Neffy® for further monitoring and additional treatment.
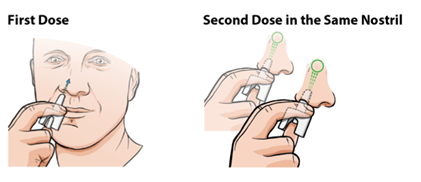
Figure 5. Administration of Neffy (Package Insert)
The most common adverse effects of nasal epinephrine include throat irritation, headache, nasal discomfort, and feeling jittery. Neffy® does not contain any contraindications. Patients with structural or anatomical nasal conditions may experience altered absorption of the nasal spray. Caution is advised in those with nasal polyps, a history of nasal fractures or injuries, or a history of nasal surgery. Clinical pharmacology studies did not include individuals with these baseline nasal characteristics, so they could not determine efficacy. In addition, those who experience allergic reactions to sulfite-containing products should understand that Neffy® contains sodium metabisulfite, which may cause allergic reactions in other products. Although Neffy® contains sulfites, individuals should not deter the use of Neffy® for treatment.
The epinephrine nasal spray should remain at 68°F to 77°F. Temperature excursions are allowed up to 122°F (50°C) but do not freeze below 5°F (-15°C). In the event the spray freezes, it will not deliver epinephrine. Persons in the austere wilderness environment should take the necessary precautions for proper storage of the product.
As a lifesaving medication, epinephrine is in most medical kits. Unique to other formulations, Neffy® provides an alternative route of administration to those who fear needles or when packing needles into a medical kit is not desired. From a safety perspective, it decreases the risk of secondhand needle sticks, ultimately increasing safety for all involved. The formulation may be advantageous in unstable environments where administering an IM injection may be challenging, or when removing enough layers to inject intramuscular formulations properly is difficult. Although there are advantages, individuals should perform a risk-benefit analysis before including intranasal epinephrine in their medical kits for the austere wilderness.
Historical note: Seasoned practitioners may remember Primatene Mist, an OTC inhaler for temporary relief of mild asthma symptoms that contained epinephrine. First sold in 1963, it was widely used for many years, but was taken off the market in 2011 because it contained CFC propellants. It was reintroduced to the market in 2018 with an HFA propellant, more environmentally friendly than the CFC. However, more effective prescription products (such as albuterol MDI) are available by prescription.