This is Part IV of a four-part series detailing some highlights of early diving physiology and medicine. This portion of the series will focus on the contributions of John Scott Haldane (Figure 1) and colleagues to the understanding of high pressure physiology and the prevention and treatment of decompression pathology in the early 20th century. See Part III in this series, Paul Bert’s Hyperbaric Contributions, for an overview of French physiologist Paul Bert’s contributions to scientific knowledge regarding decompression sickness in the late 19th century.
By 1908, Boycott et. al. would show that the tissue having the most influence on nitrogen bubble formation was fat. Nothing in Dalton’s Law - which states that the pressure exerted by a mixture of gases is equal to the sum of the partial pressure of each gas - convinced Bert’s critics that nitrogen was any more a causal agent in decompression sickness than oxygen or carbon dioxide. But Boycott et .al. proved:1) that nitrogen happens to be five times more soluble in fat than any other atmospheric gas, and 2) in a compressed air environment body fat can absorb large volumes of gas. We now know that nitrogen is constantly absorbed by adipose tissue until the partial pressure of nitrogen in fat equals the partial pressure of nitrogen in the blood (i.e., saturation is achieved). During decompression, the individual who has a great amount of adipose tissue (relative to a leaner individual) will necessarily have a greater amount of absorbed nitrogen to release – thereby having a greater risk for bubble formation and subsequent illness if the nitrogen release is fast enough, as in the case of overly-rapid decompression. The fact that a higher tissue load of nitrogen is accumulated under high pressures by those who are obese, thus heightening the risk of decompression sickness, will also be touched upon below during the discussion of John Scott Haldane’s contributions to the understanding of high pressure physiology and the prevention and treatment of decompression pathology.
Figure 1 - John Scott Haldane
Even though the etiology of decompression sickness, or the “bends” by popular terminology (so coined because of the bent posture adopted by many sufferers), was clarified by Bert, by the early twentieth century there was nothing like a proper decompression schedule that could be followed by divers - or caisson workers in a compressed air environment - in order to minimize the possibility of decompression sickness occurring. The British Admiralty was by 1900 using Royal Navy divers in its routine operations. John Scott Haldane was at this time already building a reputation in industrial applied physiology work in mining and in issues of pure science related to the physiology of breathing, particularly with questions surrounding the regulation of respiration. In 1905, Haldane, with his associate J.G. Priestley, demonstrated for the first time the importance of blood pH in determining medullary (brain stem) control of breathing, i.e., the lower the pH, the more active the medullary respiratory center. He also made significant contributions to the understanding of tissue gas physiology – notably the so-called Haldane effect whereby erythrocytes have increased ability to absorb carbon dioxide during hypoxemia or during times of increased acidity. That year, Haldane was asked by the British Admiralty to examine the problems experienced in deep-sea diving, chiefly those involving the breathing apparatuses used by divers and the so-called caisson disease (decompression sickness) they often suffered. The Royal Navy commissioned Haldane and his colleagues Dr. A.E. Boycott and Royal Navy Lieutenant Guybon Damant to work out a set of decompression schedules that could be followed by its fleet divers. Much theoretical work had already been done by Paul Bert, as well as other physiologists such as Nathan Zuntz and Leonard Hill. Haldane and his colleagues knew that the previous decompression sickness work done by Bert in particular was a very rich source from which to launch further experiments. One of Haldane’s highest priorities in preparing for studies that would take Bert’s work to the next level of discovery was the construction of a highly controlled compression chamber. With the help of the Navy, the Lister Institute of Preventive Medicine in London built a steel chamber (essentially a converted boiler little more than 2 meters long) to accommodate the work of Haldane and his colleagues. With its small windows, air lock for the passage of food, and pressure increase/decrease regulated by intricate valves and controls operated by a 24 hour a day research crew, humans and other animals could live in the chamber in relative comfort for long periods of time.
Many years before Boycott et. al. elucidated the important relationship between total body fat and nitrogen bubble formation in 1908, it had been known from anecdotal reports in humans and experimental evidence in animals that the nervous system seemed to be very frequently and most obviously affected by decompression sickness. Haldane’s microscopic examination of nerve tissue from animals subjected to rapid decompression showed bubbles restricted primarily to the (lipid-based) white matter. Furthermore, the myelin sheaths of nerves acted as “reservoirs of dissolved nitrogen”. Haldane also noted that animals that died post-decompression had 25 percent more body fat than survivors (when he analyzed total animal fatty acids). He concluded that:
Mortality runs parallel with fatness rather than with size…The practical considerations are clear…Really fat men should never be allowed to work in compressed air and plump men should be excluded from high pressure caissons or in diving to more than 10 fathoms…It is unfortunate that an increase of experience and skill in technical operations should so often be associated with the increase in waist measurement which accompanies the onset of middle life.
[Although more recent research has shown that age and VO2max may be an even bigger factor in decompression sickness than excess adipose tissue. It is widely accepted today that increasing age stimulates intravascular nitrogen bubble formation, and that a high maximal oxygen consumption suppresses bubble formation]
By 1908, there existed a reasonable understanding of the cause of decompression sickness, but it was not until this year that the scientific basis of prevention and treatment of this malady finally started to be understood (and disseminated) by investigators. Prior to this, accurately predicting the biological response in humans to decompression from a given pressure (for a given length of time) simply had not been possible. What made it possible, by 1908, to formulate the basis from which a modern decompression system would be built were the many hundreds of tests on animals and humans that Haldane and his colleagues commenced in 1903.
It can be argued that it was Haldane and company’s study of goats (in particular) in an environment that permitted experimental compression and decompression - because they are easily handled and have a fat-blood distribution similar to humans - that allowed him to produce the first set of practical decompression schedules in 1908. They knew that fatty tissues, able to absorb 5 times more nitrogen than other tissues, with the poorest blood flow were not only the last tissues to fully saturate when compressed to a higher pressure, but were the last tissues to fully desaturate when decompressed. These investigators were ultimately able, through extensive experimentation, to quantify this time: depth relationship. It can arguably be said that Haldane and his collaborators’ most significant role in the advancement of diving physiology and hyperbaric medicine stemmed primarily from: 1) finding that decompression sickness symptoms increased steadily over time relative to subjects’ depth and time at depth prior to decompression until a plateau was reached and the symptoms no longer worsened with even more extended times at depth (suggesting complete nitrogen saturation of the body), and 2) the more saturated with nitrogen a tissue became, the more time it took for tissue desaturation to lessen the chance for pathological bubble formation.
Haldane’s team eventually demonstrated that a 2:1 reduction in ambient pressure was possible to achieve without bringing on the symptoms of decompression sickness. Therefore, if a diver had spent time at a depth of 20 m, he could be brought up to 10 m without danger. Likewise, someone diving at 40 m could rapidly ascend to 20 m, and so forth.
This gave rise to Haldane’s theory of tissue half-times – that the likelihood of developing bubbles to cause decompression illness was proportional to the amount of nitrogen dissolved in the tissue with the slowest ability to desaturate to a nitrogen tension that was one-half of its supersaturated state. Fatty tissues have, therefore, a longer half-time than more watery tissues like muscle.
After halving the pressure on ascent, Haldane found that the diver needed to spend adequate time at this stop in order to permit excess nitrogen to be eliminated from the body. After a calculated period of time, the diver could then ascend to the next stop. Not surprisingly, this was termed “stage decompression” (actually as early as 1878 by Paul Bert). Bert preferred continuous ascent at a constant speed, however, simply because he considered it more practicable. Haldane, to the contrary:
helped establish this concept [stage decompression] as the standard decompression procedure, thus not only introducing a safer decompression strategy, but also reducing the overall decompression time considerably. The uniform decompression method [continuous ascent at a constant speed], according to Haldane, wastes too much time.
Uniform decompression was shown to be dangerous, chiefly because it did not fully consider tissues of the central nervous system which have a high fat content and thus release nitrogen more slowly. Boycott et. al stated:
This slowness has never hitherto been recognized but must evidently be reckoned with in devising measures for the prevention of caisson disease…It [uniform decompression] is needlessly slow at the beginning and usually dangerously quick at the end… On the other hand, decompression should…be as rapid as possible, consistent with safety.
In human decompression experiments from pressures as high as 6.4 atmospheres, often with Haldane and his colleagues acting as research subjects, which included Haldane’s own young son, JBS, as one of the subjects (who would later become arguably even more famous than his father in the scientific world), the hypothesis of stage decompression held true. However, it quickly became obvious that for deep dives of long duration, even Haldane’s decompression schedule could be exceedingly slow – especially when it was impractical or dangerous to ascend from the depths in such a deliberate manner (e.g., in cold water where hypothermia was a distinct concern). This led to the development of specialized recompression chambers by Sir Robert Davis just a few years prior to the outbreak of World War I.
Davis designed a cylindrical steel chamber big enough to hold two people. A trap door in the bottom of the chamber was provided through which a diver could enter when the chamber was lowered into the water (Figure 2). The chamber was kept full of air and properly ventilated by compressed air conveyed through a pipe from the surface. The chamber, with an attendant inside it, was lowered to a depth corresponding to an early stage of the diver’s stage decompression. Upon ascending to this stage, the diver entered the chamber (Figure 3a), which was then closed. The further stages of decompression were then completed within the chamber while it was being hauled up to the deck of the ship. To hasten the decompression, the diver was given supplemental oxygen to breathe as soon as the pressure was low enough to safely allow it (Figure 3b).
It was later learned that a diver could, in many circumstances, ascend to the surface in rapid fashion and then immediately climb into a recompression chamber (often on a ship) - to be quickly recompressed to “depth” for a slow staged decompression. Decompressions of this nature are now a routine part of military and commercial diving.

Figure 2 – Davis decompression chamber ready for use. From Haldane and Priestley’s Respiration (1935).

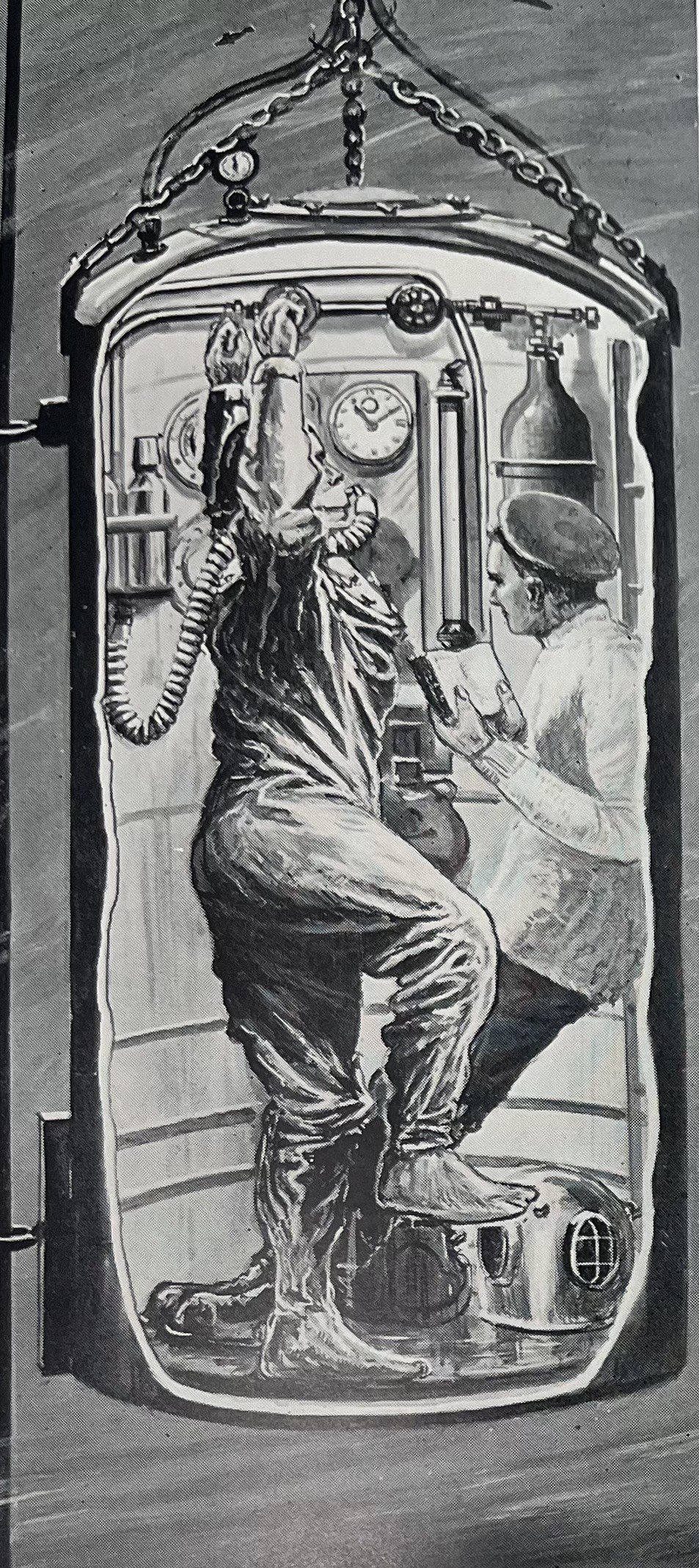
Figure 3a Figure 3b
In Fig 3a the diver enters the Davis decompression chamber underwater. In Fig 3b the diver is breathing oxygen and exercising to accelerate removal of nitrogen. From Haldane and Priestley’s Respiration (1935).
Haldane and his colleagues’ realization that body tissues absorb nitrogen at varying rates depending on their vascularity and the type of tissue involved was of tremendous importance when developing the calculations for decompression "stop" durations during ascent. The decompression tables developed by Boycott et al. in 1908:
became the standard of their time for diving operations throughout the world, drastically reducing the number of decompression fatalities. They still provide the basis for modern decompression algorithms used in diving computers and diving tables found in commercial, recreational, and military diving.
The diving tables used today all incorporate the first stage of decompression introduced to the world in 1908, i.e., halving the pressure immediately with rapid ascent. Perhaps not surprisingly, however, much “fine-tuning” has been done to the dive tables over the years, especially for the long and deep dives often carried out for military and commercial objectives. Most notably, extra decompression time and decompression stops have been added for long dives to extreme depths, aside from the altered gas mixtures divers must breathe at great depths to avoid nitrogen and oxygen toxicity. Correspondingly, surface chambers for recompression and decompression, and the scientific basis for their use, have become more sophisticated as the need for very long decompression times has become a fact of life for many military and commercial divers.