
Introduction
Wounds and lacerations are common, resulting in significant morbidity in civilian settings, military conflicts, and wilderness areas that often require medical evacuation. Approximately 12 million patients visit US emergency departments each year for wound closure. Wound infection is the most prevalent complication, occurring in 2.5% of sutured wounds. Wound irrigation reduces the risk of infection by removing foreign materials, decreasing bacterial contamination, and clearing away cellular debris. Vigorous irrigation is essential but not excessive to prevent tissue trauma or push bacteria deeper into the wound. The Wilderness Medical Society (WMS) provides a Clinical Practice Guideline (CPG) for basic wound management for skin and soft tissue injuries (SSTIs), which includes proper wound preparation and water irrigation to promote healing. Refer to Table 1 below for CPG recommendations on wound irrigation for common wilderness injuries and the supporting evidence.
Table 1. Wound Preparation and Irrigation (Quinn et al.)
|
Recommendations
|
Strength of Evidence*
|
|
An attempt at wound cleansing is recommended in the presence of high bacterial contaminants and dirt.
|
Strong recommendation, low-quality evidence
|
|
A foreign body composed of reactive or contaminated material should be removed in the field if removal can be performed easily and with a low risk of complication.
|
Strong recommendation, low-quality evidence
|
|
Wounds should be treated using a clean field, including gloves and instruments; sterility is not necessary.
|
Strong recommendation, high-quality evidence
|
|
The use of high-pressure irrigation (6–12 psi)** is recommended to lower wound infection rates, especially in the case of open fractures.
|
Strong recommendation, high-quality evidence
|
|
Irrigation should be performed as quickly as practical as there is a direct correlation between timing and effectiveness of irrigation.
|
Strong recommendation, moderate-quality evidence
|
|
Irrigation should include at least 1 L of irrigant.
|
Strong recommendation, low-quality evidence
|
|
In a wilderness setting, potable water is the preferred solution for wound irrigation.
|
Strong recommendation, high-quality evidence
|
|
If irrigation is performed, additives should not be used (except for rabies-prone wounds).
|
Strong recommendation, high-quality evidence
|
* Strength of evidence based on GRADE methodology from American College of Chest Physicians, 2018. Recommend high pressure (6-15 psi) is more effective than low pressure (<6 psi) to remove bacteria and foreign debris
Managing SSTIs typically requires wound irrigation with sterile saline, which may necessitate large volumes based on the degree of tissue damage. However, the availability of sterile fluids needed may be limited depending on the environment and logistics. Current recommendations for irrigation volumes, as outlined in a Clinical Practice Guideline by the Joint Trauma System, are as follows:
- 1-3 liters for small-volume wounds
- 4-8 liters for moderate wounds
- 9 or more liters for severe wounds or those with significant contamination
However, water quality and volume limitations may hinder effective wound irrigation in severely contaminated wounds in austere settings, as the necessary fluid amounts are impractical for personnel to carry. Normal saline, sterile water, and potable tap water exhibit comparable efficacy and safety. Furthermore, a Cochrane review suggested that potable water can replace sterile water without negatively impacting infection outcomes. In resource-limited environments, treated groundwater with proper decontamination could be the only option for managing severely contaminated wounds, especially when extended care (days rather than hours) is needed due to delayed evacuation in austere settings. Note: The Joint Trauma System CPG states that the addition of additives in irrigation fluid, e.g., povidone-iodine solution, bacitracin, or antibiotics, has no proven benefit.
To address this limitation, a study by Holcomb et al. evaluated the effectiveness of commercial water treatment methods for decontaminating water used in wound irrigation. They aimed to compare six common water purification methods to determine which was more effective than the chlorine purification method (CHLOR-FLOC), the military's standard for water purification since the 1940s. As outlined, they assessed six water purification techniques across seven critical variables to identify their optimal application in austere environments. These variables included bacterial culture, pH, turbidity, cost, flow rate, and device size. Their evaluation established the most effective method that is:
- The most convenient for field transportation;
- The most effective in treating contaminated water;
- The most durable during field usage;
- The most rapid method for producing an adequate volume for wound irrigation.
These purification systems were categorized by mechanisms of purification: 1) chemical methods, 2) filtration/ultraviolet light, and 3) thermal. The chemical purification methods used were: 1) Aquamira Water Treatment drops, 2) Potable Aqua Water Purification Germicidal Tablets, and 3) The CHLOR-FLOC water purification sachets. The filtration/ ultraviolet light methods included: 1) Steripen Ultralight and Steripen FitsAll Filter and 2) The Guardian purifier. The sixth method used was boiling (100°C/212°F for 3 minutes), considered the gold-standard water disinfection technique.
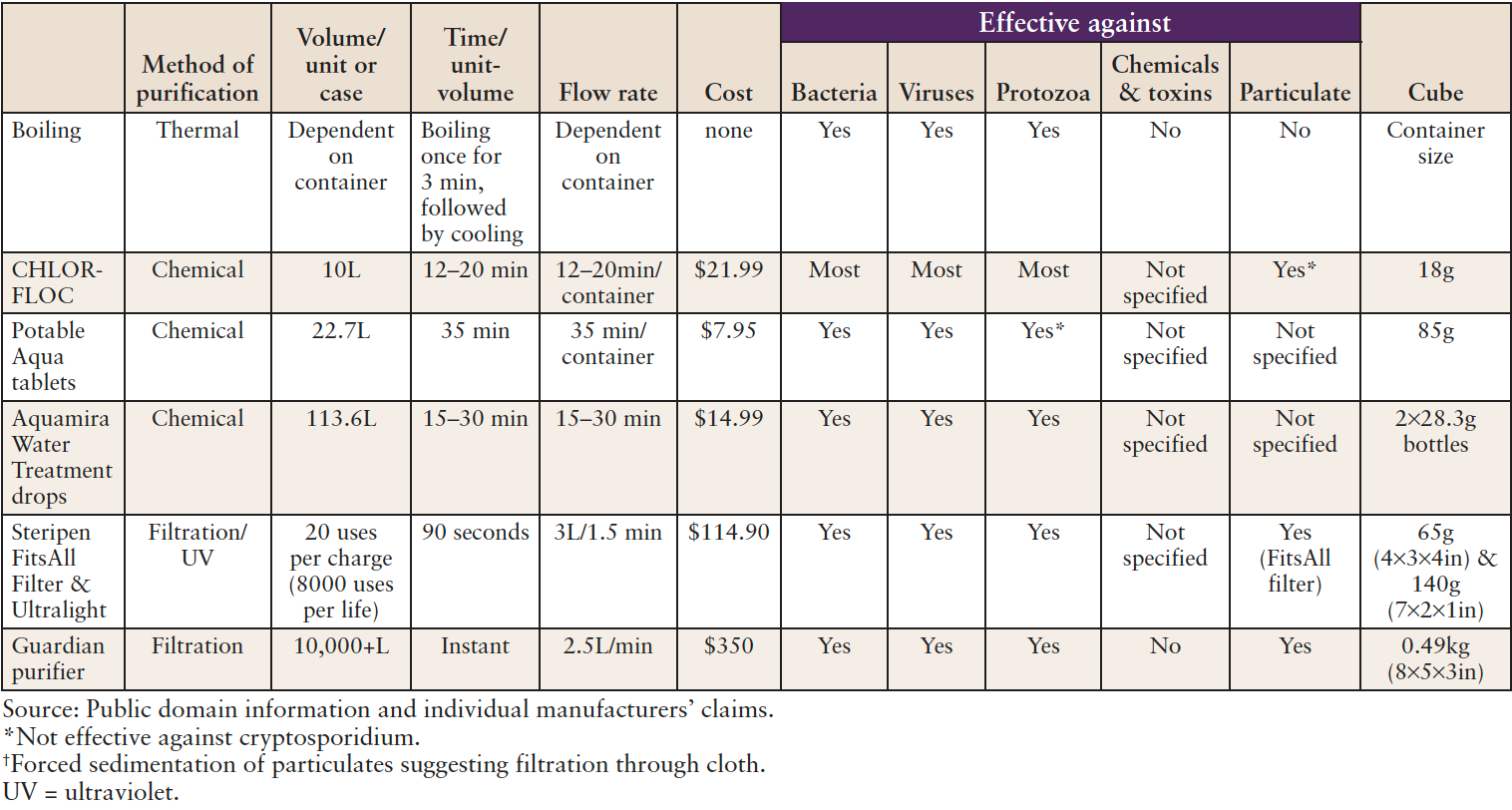
Despite the absence of a universally optimal water decontamination method across all six study parameters, it was concluded that no single device demonstrated perfect performance. Each method showed both perceived strengths and weaknesses. This observation was based on the fact that all methods employed (chemical, filtration/ultraviolet, and thermal) effectively reduced microbial levels. The results of the current study should be interpreted in light of several limitations, as stated by the authors. They only evaluated bacterial load and did not include tests for viruses, protozoa, chemicals, and toxins, and they relied solely on the manufacturer’s descriptions. Notably, CHLOR-FLOC has many desirable characteristics and effectively reduces the microbial load in contaminated water. In austere settings where all equipment is manually carried, the Aquamira drops appear superior to other small, lightweight products, given their high-volume throughput, low cost and size, and positive effects on pH and water decontamination within 15-30 minutes. At a much higher cost but still providing a high volume of water in a shorter timeframe, the Steripen and FitsAll filter produced 3 liters in 90 seconds, while the Guardian purifier generated 2.5 L/minute. See Table 2 for key criteria and outcomes of the studied water purification systems.
Table 2: Key Criteria and outcome for six water purification systems used in Holcomb et al.
Application to the Wilderness Medicine Provider
Ideally, any water decontamination method chosen should effectively remove water turbidity, bacteria, and viruses while producing sufficient quantities of potable water for individual or group use for oral hydration and, when necessary, for wound irrigation. Key takeaways for wilderness providers and individuals in remote settings, such as backcountry camping or disaster-stricken populated areas, where the injured may experience delayed wound closure until definitive care, should utilize at least one liter or more, depending on the severity of the wound. It is advisable to be prepared with two to three water decontamination options, including boiling water, chemical treatments such as Aquamira water treatment drops, and ultraviolet/filtration methods. Boiling water remains the most reliable method for eliminating microorganisms. However, if boiling water is not feasible, a filter is the next most effective option to reduce water turbidity or cloudiness. Subsequently, a Steripen can be employed to eliminate bacteria and viruses. It is important to note that Steripens are less effective in cloudy water, necessitating the use of a FitsAll™ filter. Commercial water filters do not remove viruses unless the filter’s pore size is at least 0.2 microns or smaller.
We concur with the findings of Holcomb et al. that a layered approach to water purification is optimal, given the substantial number of individuals who require daily hydration through a single commercial product and the volume of water necessary for wound irrigation. Based on criteria such as the gear carried, cost-effectiveness, size/weight, the capacity to produce a high volume of water, efficacy for water decontamination, and pH, Holcomb et al. recommend Aquamira drops. However, a Guardian purifier filter is suggested when cost is not a primary consideration. Finally, the findings by Holcomb et al. align with recommendations provided by the US Centers for Disease Control and Prevention and the Wilderness Medical Society Clinical Practice Guidelines on water decontamination for drinking water.
Author (BB) Note: I prefer water filtration devices like Sawyer, MSR, Katadyn, or Guardian for personal hydration in the field. I also carry Portable Aqua tablets as a chemical backup. For international city travel in developing countries, I use Steripen for non-turbid water. These methods quickly provide over a liter of water for initial wound irrigation.