Introduction
The Amazon rainforest, with its vast rivers and remote communities, presents unique challenges to healthcare professionals. In these isolated environments improvisation, adaptability, and quick decision-making become essential as access to advanced medical resources is limited. This article recounts the experience of treating a 12-year-old girl who suffered a fish bite that progressed to necrosis, underscoring the life-saving principles of wilderness medicine.
The Incident
One afternoon, a 12-year-old girl from a riverside community along the Rio Purus was brought to our remote village clinic in Fazenda São Sebastião. While swimming in the river, she had been bitten by a Candiru-açu (Cetopsis candiru), a fish known for inflicting deep wounds with its sharp teeth. Initially, the wound on her lower leg appeared to be a minor laceration. However, given the region’s heat, humidity, and the presence of waterborne bacteria, infection was a significant concern.

Figure 1: Map of Rio Purus and the location of the clinic.
Using wilderness medicine principles, I conducted an initial evaluation with the M.A.R.C.H. protocol (Massive hemorrhage, Airway, Respiration, Circulation, Hypothermia prevention). There were no immediate life-threatening issues, and the patient was alert but exhibited signs of mild dehydration. After irrigating the wound with the cleanest water available, I dressed it with sterile gauze and started her on oral antibiotics (amoxicillin-clavulanate). Pain relief was provided with oral analgesics, and we advised her family to monitor her condition closely.
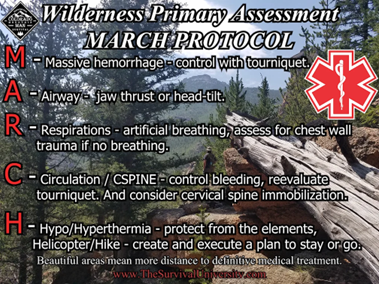
Figure 2: MARCH protocol acronym
Signs of Complication and Refusal of Evacuation
Within 48 hours, the patient’s condition deteriorated. Her leg became swollen and erythematous, with areas of the wound turning black—a clear sign of necrosis. She also presented with fever and symptoms of dehydration, including dry mucous membranes and poor skin turgor. Given the severity of her condition, immediate surgical intervention was necessary to prevent further complications.
We recommended transferring her to the nearest hospital, a multi-day boat journey, for advanced care. However, the patient and her family refused evacuation, opting to remain in their community. Their decision reflected deep cultural and emotional ties to their environment, which we respected. This meant we had to perform the debridement on-site to save her life.
We established intravenous (IV) access and administered normal saline to address her dehydration. With her condition stabilized, we prepared for the procedure.

Figure 3: Renata Macedo Soares, Dr. Ciro Campos, Dr. Liz Matzenbacher, and Dr. Daniel Juliano Rezende during our first arrival at the patient's home after the family's call. Photo by Dr. Carlos Henrique Aragão Neto.
The Debridement: A Life-Saving Procedure in the Wilderness
Performing a debridement in a remote jungle setting, far from the sterile conditions of a hospital, required improvisation. We sterilized the instruments over an alcohol burner, and with the help of local volunteers, we set up a makeshift sterile field. Lidocaine was administered for local anesthesia, although we knew it would provide only limited relief.
Step by step, I excised the necrotic tissue while preserving as much healthy skin as possible. Between cuts, the instruments were cleansed with boiled water. Despite the challenges—the heat, humidity, and emotional weight of treating a young patient—our teamwork and trust with the family allowed the procedure to be completed successfully.

Figure 4: Dr. Daniel Juliano Rezende performing a debridement procedure on the patient. Photo by Dr. Ciro Campos.
Post-Operative Management and Recovery
After the debridement, we continued her on antibiotics and IV fluids to prevent reinfection and support recovery. Dressings were fashioned from gauze soaked in a homemade saline solution, and we trained her family to manage the wound and monitor for signs of reinfection. In wilderness medicine, empowering caregivers is essential, as follow-up care may be limited. Over the following days, the patient’s condition improved. Granulation tissue began to form, indicating that the wound was healing well. The patient’s resilience, combined with the dedication of her family, was critical to her recovery.

Figure 5: Renata Macedo Soares collecting patient data while the patient receives intravenous analgesic therapy. Photo by Dr. Carlos Henrique Aragão Neto.
Lessons Learned
This case exemplified several key principles of wilderness medicine:
- Respect for Cultural Sensitivity and Patient Autonomy: The family’s choice to stay in their community presented a unique challenge. Adapting our treatment to respect their decision not only showed our commitment to the patient’s health but also honored her family’s connection to their environment. This cultural sensitivity strengthened our rapport and ensured a more supportive recovery process. Such respect for autonomy is critical in remote medicine, where traditional beliefs and values often influence healthcare decisions.
- Improvisation and Adaptability: Without access to a fully equipped surgical setup, we had to transform a basic clinic into a viable operating space. Improvisation became a core skill, from sterilizing instruments over an alcohol burner to creating a makeshift sterile field in the heart of the jungle. This experience underscored the necessity of adaptability and quick thinking to meet the pressing demands of patient care when traditional tools and techniques are out of reach.
- Importance of Early Recognition and Management of Dehydration and Infection: In wilderness settings, early intervention is vital for preventing complications. Recognizing signs of dehydration and infection allowed us to stabilize the patient before proceeding with the surgical intervention. This experience highlighted the value of vigilant assessment and immediate treatment, even with limited resources, to manage potentially life-threatening complications.
- Empowering Local Community for Ongoing Care: Given the lack of regular follow-up, empowering the patient’s family to manage post-operative care was essential. Teaching basic wound care techniques and infection monitoring transformed her caregivers into key participants in her recovery. This collaborative approach not only ensured continuity of care but also built resilience within the community to handle similar cases in the future.
- The Role of Teamwork and Emotional Resilience: Performing a debridement on a young patient, far from hospital resources, tested not only clinical skills but also emotional resilience. The gravity of her condition, coupled with the intense environment, reminded us that practicing medicine in remote areas requires mental fortitude, as well as trust and teamwork with those present. This shared responsibility made a challenging situation manageable and underscored the power of collective effort in overcoming medical emergencies.

Figure 6: Exterior of the patient's house in the Fazenda São Sebastião village. Photo by Dr. João Claudio Lyra.
Conclusion
Practicing medicine in the Amazon tested the limits of my skills and reinforced the importance of adaptability, teamwork, and compassion. In environments far from modern infrastructure, we relied not only on clinical knowledge but also on trust and creativity to save lives. This experience deepened my understanding of the essence of wilderness medicine: to provide care wherever it is needed, no matter the challenges.