
Coiled rattlesnake. Photo by poison.org
In May of this year, two-year-old Brigland Pfeffer ran to his mother, Lindsay, holding his right hand. Confused about what was bothering her son, Lindsay spotted a faint drop of blood on his finger but was unable to determine any cause. Moments later, Brigland’s brother shouted that he saw a snake, and Lindsay confirmed that a small rattlesnake was lying by their firepit. 911 dispatch directed the Pfeffers to wait for an ambulance and they were taken 25 minutes away to the Palomar Medical Center in Escondido. By the time Brigland arrived at the hospital, his hand and arm were severely swollen and purple. Brigland received his starting dose of the antivenom Anavip, an antivenom made of equine-derived antibody fragments. Brigland received 30 vials of Anavip; the initial dose of 10 was administered at Palomar, and the subsequent 20 were given to him at Rady Children's Hospital in San Diego. The cost of his hospital stay and antivenom treatment was $297,461.
Venomous snakes in the United States come from two scientific families: Elapidae and Viperidae. A subfamily of Viperidae, Crotalidae (pit vipers), make up 99% of envenomations in the United States and are comprised of rattlesnakes, copperheads, and cottonmouths. Bites from pit vipers are treated with the antivenoms CroFab or Anavip. Use of antivenom is indicated based on the presence of progressive local tissue damage, coagulopathy, or systemic effects. For known crotalid envenomations, the Snakebite Severity Score helps guide the initiation of antivenom. CroFab and Anavip require an initial loading dose (4-6 vials for CroFab and 10 vials for Anavip) and are subsequently dosed based on patient improvement. Different factors dictate the severity of envenomation, which results in a lack of standardization regarding how many vials will be needed to treat a specific patient. Of note, dosing does not differ between pediatric and adult patients.
An analysis on the use of CroFab and Anavip for rattlesnake envenomations from 2019-2021 showed the mean number of vials of antivenom per patient differed between the two; CroFab received 10.19, and Anavip received 19.98. In this analysis, the highest number of vials of Anavip given was 25, five vials short of the total Brigland received. A retrospective review from 2022 identified a range of 8-30 vials of Anavip, with the mean being 16, required to achieve symptom control. The Anavip package insert advises repeated hourly dosing until local signs of envenomation are no longer progressing and “there is no known maximum dose.”
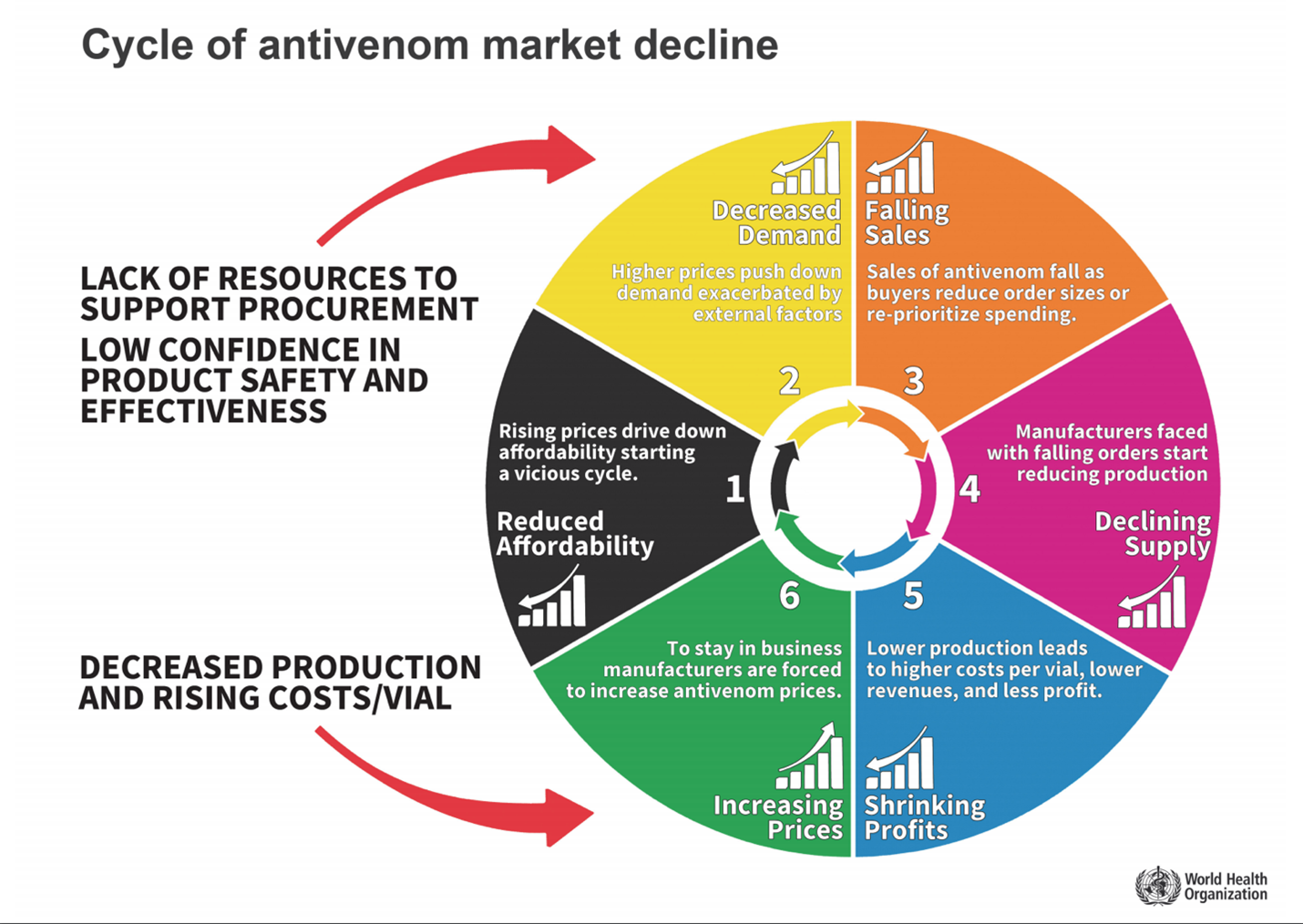
Cycle of antivenom decline. Photo by WHO.int
The World Health Organization (WHO) cites a vicious cycle and relationship of cost, demand, and supply that continues to stifle the antivenom market and perpetuate the low availability and high-cost predicament. There may, however, be hope on the horizon. Current treatment methods rely on polyvalent antivenoms, like CroFab and Anavip, comprised of antibody fragments from immunized animals. These fragments lack venom specificity, resulting in the potential need for multiple treatments, and because they come from other animals, they have the potential to cause serious side effects. Recombinant antivenom, currently in development, is created by synthesizing human antibodies in a laboratory. These are generally much more specific to the venom they target and can be delivered at more therapeutic concentrations without the risk of adverse reactions inherent to receiving animal antibodies. One of the best aspects of this new antivenom is its anticipated affordability. Scientists estimated that one complete antivenom treatment could cost as low as $60 based on industrial cost estimates of antibody expression.
Snake envenomation continues to loom as a globally significant source of morbidity and mortality. In the case of Brigland Pfeffer, it is evident how important it is to have access to the appropriate treatment and get there as quickly as possible. Brigland's example also highlights the disparity between the United States and the rest of the world when comparing snake envenomation fatalities. According to the Wilderness Medical Society (WMS) Clinical Practice Guidelines (CPG) on Pitviper Envenomations, “all venomous snakebites should be evacuated and transported to the nearest emergency department. Rapid transport to an emergency department allows for life- or limb-saving interventions.” Awareness allows for quick action to be taken in the event of an emergency. You can find out which facilities nearest you have antivenom by contacting your poison control center (1-800-222-1222).